Small Bowel Obstruction
SBO
· General considerations
o Small bowel obstruction, as the term is used here, is due to physical and organic changes which produce mechanical obstruction to the passage of the bowel contents somewhere in the small bowel
o The bowel proximal to the point of obstruction dilates with swallowed air and secreted fluid,
§ Vomiting may release some of the proximal bowel contents and reduce the amount of proximal dilation
o The bowel hyperperistalses
o Bowel distal to the point of obstruction (i.e. colon and sometimes distal small bowel) empties over time
o Strangulation of the bowel may result from vascular compromise of the affected loops and is a cause of increased mortality
· Causes
o Overwhelmingly, the most common cause of a mechanical small bowel obstruction are adhesions related to prior surgery (60%)
§ The most common prior surgeries associated with a subsequent SBO include appendectomy, colorectal surgery and gynecologic surgery
§ Bowel may become kinked under an adhesion
§ The obstruction is frequently partial or intermittent
o Hernias
§ Most often femoral or inguinal
o Intussusception
o Volvulus
o Tumor, either primary or metastatic
o Wall lesions such as leiomyomas or strictures
o Crohn’s disease
o Foreign bodies
o Gallstones
§ Such as in gallstone ileus (which is actually a mechanical obstruction, usually at the ileocecal valve)
· Clinical findings
o Abdominal pain and distension
§ Most marked in patients with distal SBO although its onset in distal obstructions is later in the course of the disease than in proximal obstruction
§ Typically colicky in nature and progressively worsening over time
o Nausea
o Vomiting
§ An earlier sign of a proximal than a distal obstruction
§ Fluid and electrolyte imbalances from vomiting increase mortality
o Constipation
o History of prior abdominal or pelvic surgery
o Bowel sounds are hyperactive and high-pitched
§ Absence of bowel sounds may indicate bowel ischemia or peritonitis
· Imaging findings
o Conventional radiography is the study of first choice
§ Loops proximal to the point of obstruction will become dilated and fluid-filled
· Usually greater than 2.5-3 cm in size
§ Differential height of air-fluid levels in the same loop of small bowel no longer considered reliable sign of mechanical SBO
§ Absence of, or disproportionately smaller amount of, gas in the colon, especially the rectosigmoid
§ Loops of small bowel may arrange themselves in a step-ladder configuration from the left upper to the right lower quadrant in a distal SBO
§ Mostly fluid-filled loops of bowel may demonstrate a string-of-beads sign caused by the small amount of visible air in those loops

Small Bowel Obstruction. Supine view of the abdomen (left) shows several dilated loops of small bowel
in the upper abdomen. The small bowel is disproportionately dilated compared the the large bowel
which is collapsed. The upright view (right) demonstrates multiple air-fluid levels in the dilated loops
in a typical configuration of a small bowel obstruction. The patient had previous bowel surgery.
For a larger photo of the same image, click here
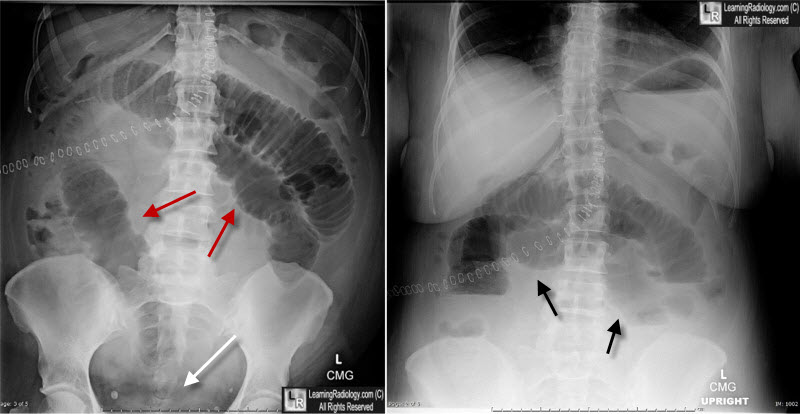
Small Bowel Obstruction. Supine view of the abdomen (left) shows multiple dilated loops of small bowel
in the upper abdomen (red arrows). The small bowel is disproportionately dilated compared the the large bowel
which is collapsed. There is no air in the rectosigmoid (white arrow). The upright view (right) demonstrates multiple air-fluid levels in dilated loops of a small bowel obstruction. The patient had previous bowel surgery.
o CT may demonstrate the site and cause of the obstruction
§ Dilated and fluid-filled loops of small bowel proximal to the obstruction and collapsed loops of small bowel and/or colon distal to the obstruction
§ Small bowel feces sign is seen in SBO because of the intermixing of air with material that is static in obstructed small bowel, resembling the appearance of feces
§ While adhesions are not imaged per se, their presence can be inferred by a rapid change in bowel caliber without any other causes of obstruction (e.g. tumor) suggested
§ Signs of strangulation include thickening of the bowel wall, increased attenuation of the bowel wall, stranding of the adjacent small bowel mesentery or pneumatosis intestinalis
§ CT may demonstrate tumors, Crohn’s disease, gallstone ileus, hernias, closed loop obstructions which are usually not diagnosable on conventional radiographs
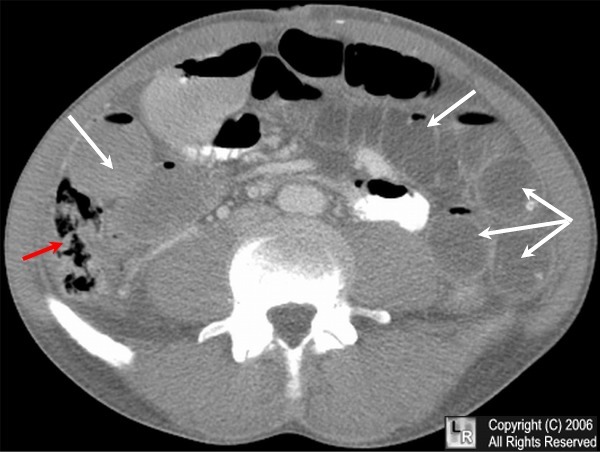
CT of Small Bowel Obstruction. Axial CT scan through the lower abdomen shows
multiple fluid-filled and dilated loops of small bowel (white arrows) and collapsed
right colon (red arrow) consistent with a mechanical small bowel obstruction.
· Closed-loop obstructions
o Most (75%) are caused by adhesions
o In a closed-loop obstruction, the twisted loop itself remains dilated with gas and fluid thus producing a dilated, U-shaped loop of small bowel
§ Does not change in position or size over time
· Coffee bean sign or pseudotumor may be seen
o Closed-loop obstructions are not usually diagnosable by conventional radiography and require CT
§ CT findings may include a U- or C-shaped loop of small bowel
§ A spoke-like configuration of the mesentery demonstrating stretched vessels converging on the site of the twist may be seen
· The appearance of the tightly twisted mesentery has been called the whirl sign
§ The beak sign may be seen as a fusiform tapering at the site of the obstruction
· Treatment of small bowel obstruction
o Many patients are treated conservatively with small bowel decompression and intravenous fluids
o Surgical intervention may be necessary if there are signs and symptoms of strangulation, peritonitis or lack of response to conservative treatment
Differentiating SBO from Paralytic Ileus |
|
SBO |
Ileus |
Etiology |
Patient with prior surgery weeks to years prior |
Recent (hours) post-operative patient |
Pain |
Colicky |
Not a prominent feature |
Abdominal distension |
Frequently prominent |
Sometimes not apparent |
Bowel sounds |
Usually increased |
Usually absent |
Small bowel dilatation |
Present |
Present |
Large bowel dilatation |
Absent |
Present |
|
