|
Pulmonary Thromboembolic Disease
· Age
o Usually occurs
after 60 years of age
· Cause
o Most common
cause is deep vein thrombosis
(DVT) of lower extremity in
>90%
· Predisposing
factors
o Immobilization
(56%)
o Surgery (54%)
· Pathophysiology
o Clot from deep
veins of leg breaks off
o Travels via
venous system to right side of
heart
o Fragments in
right side of heart
o Showers lung
with emboli varying in size
§ On average > 6-8
vessels are embolized
· Clinical
findings
o Hemoptysis
(25-34%)
o Pleural friction
rub
o Thrombophlebitis
§ But only about
10-33% of patients with fatal
pulmonary embolism (PE) are
symptomatic for DVT
o Acute dyspnea
(81-86%)
o Pleuritic chest
pain (58-72%)
o Apprehension
(59%)
o Cough (54-70%)
o Tachycardia
o Tachypnea
o Accentuated 2nd
heart sound
o EKG changes
(83%)
§ Mostly
nonspecific
o Elevated levels
of fibrinopeptide-a (fpa)
= small peptide split off of
fibrinogen during fibrin
generation
o Positive d-dimer
assay (generated during clot
lysis)
· Location of
pulmonary emboli
o Bilateral emboli
in 45%
o Right lung only
in 36%
o Left lung only
in 18%
o Multiple emboli
[3-6 on average] in 2/3
· Distribution
by lobe
o Lower lobes more
often than upper lobes
o RUL (16%)
o RML (9%)
o RLL (25%)
o LUL (14%)
o LLL (26%)
· Site ─
central versus peripheral
o Central =
segmental or larger veins in
58%
o Peripheral =
subsegmental or smaller veins
in 42%
o In subsegmental
branches exclusively in 30%
o Emboli are
occlusive in 40%
· Resolution of
pulmonary embolism
o Through
fibrinolysis and fragmentation
o By time interval
§ In 8% by 24
hours
§ 56% by 14 days
§ 77% by 7 months
o By completeness
§ Complete in 65%
§ Partial in 23%
§ No resolution in
12%
§ Resolution less
favorable with increasing age
and cardiac disease
· Embolism
without infarction (90%)
o Dual blood
supply of lungs ─ pulmonary
and bronchial
· Imaging
findings in embolic disease
without infarction
o Normal chest
film common
o Normal chest
x-ray has a negative
predictive value of only 74%
o Plate-like
(subsegmental, discoid)
atelectasis
o Lobar
consolidation in lower lung
zones and pleural effusion
(most common findings with the
lowest positive predictive
value)
o Westermark sign represents an area of oligemia
(due to vasoconstriction
distal to embolus)
§ Uncommonly seen

Axial CT image just below level
of tracheal bifurcation
demonstrates large
intraluminal filling defects
in both right and left
pulmonary arteries representing a "saddle
embolus" straddling
the pulmonary arteries.
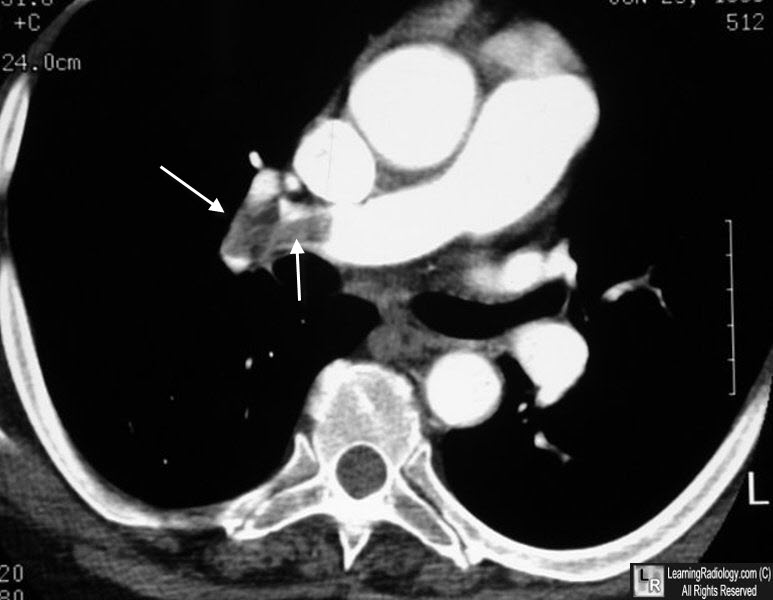
Pulmonary embolism. There is a large filling defect (white arrows) in the right pulmonary artery representing clot.
o Fleischner sign
refers to local widening of
artery by impaction of embolus
(due to distension by clot /
pulmonary hypertension
developing secondary to
peripheral embolization)
o "Knuckle sign"
is term used for abrupt
tapering of an occluded vessel
distally
· Imaging
findings in embolism with
infarction
o Segmentally distributed
wedge-shaped consolidation
(54%)
§ With or without
cavitation
o Hampton hump is
a pleural-based area of
consolidation in the form of a
truncated cone with base
against pleural surface
o Pleural effusion
in slightly over 50%
§ Thoracentesis
· Bloody (65%)
· Predominantly
PMNs (61%)
· Exudate (65%)
o Usually no
air-bronchogram because of
hemorrhage into alveoli
o "Melting sign"
is the sign that refers to
disappearance of the
opacification within few days
to weeks from periphery toward
center
o Fleischner lines
= long-line shadows (fibrotic
scar)
o Plate-like
(subsegmental, discoid)
atelectasis (27%)
o Cardiomegaly or
CHF (17%)
o Elevated
hemidiaphragm (17%)
o Subsequent
nodular or linear scar more
often than pneumonia leads to
scarring
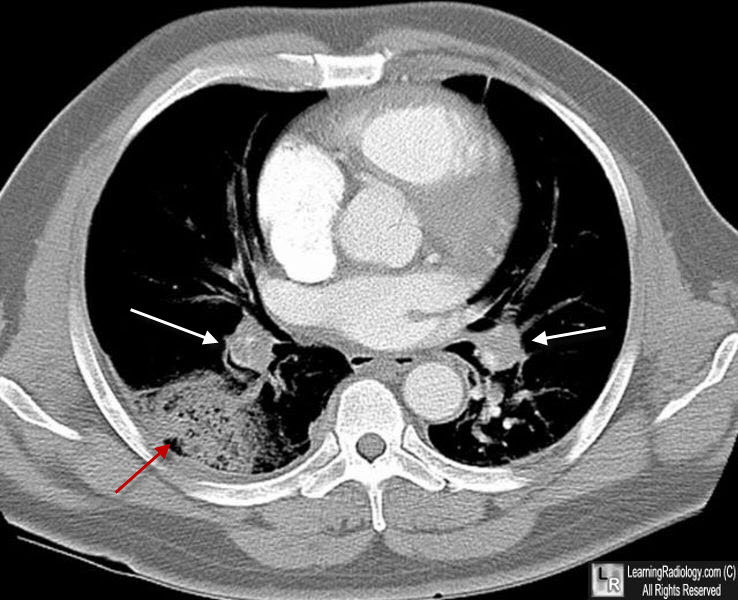
Hampton Hump. Axial CT scan of the chest shows bilateral filling defects in both pulmonary arteries (white arrows) representing thrombi. There is a large, wedge-shaped, pleural-based soft tissue density that represents the infarct and is called a Hampton Hump.
· CT findings (can be equal to angio in
detection of emboli within
proximal arteries):
o Subsegmental
intraluminal filling defects
may not be detectable
o Detection is
poorer in middle lobe and
lingular branches
o Peripheral
wedge-shaped lung densities
with the triangle base
adjacent to pleural surface
o Peripheral
rimlike contrast enhancement
in a pulmonary artery
o Intraluminal
filling defect in pulmonary
artery
· NUC (VQ scan =
guide for angiographic
evaluation)
· Interpreted in
reference to Biello or PIOPED criteria
o Low- /
intermediate-probability scans (73%)
§ Additional
studies recommended
o High-probability
scan
§ In 12% normal
angiogram
· Angiographic
findings
o Intraluminal
defect (94%)
o Abrupt
termination of pulmonary
arterial branch
o Pruning and
attenuation of branches
o Wedge-shaped
parenchymal hypovascularity
o Absence of
draining vein in affected
segment
o Tortuous
arterial collaterals
o Complications of
pulmonary angiography
§ Arrhythmia,
endocardial injury, cardiac
perforation, cardiac arrest,
contrast reaction
|
