|
|
Right Upper Lobe (RUL) Atelectasis
General Considerations
- All types of atelectasis involve loss of volume in some or all of a lung with resultant increased density of the involved lung
- The atelectasis referred to here is that caused by bronchial obstruction, usually a tumor (i.e. a bronchogenic carcinoma), a foreign body or a mucus plug
- Right upper lobe (RUL) atelectasis in adults is more often caused by a tumor than a mucus plug
Imaging Findings
- On the frontal view of the chest, elevation of the minor fissure associated with increased density of the right upper lobe which migrates medially and superiorly towards the apex of the lung
- If the atelectasis is caused by a hilar mass obstructing the RUL bronchus, the shape of the mass and the retracted minor fissure may resemble a “reverse S” (Sign of Golden)
- There may be elevation of the right hilum and tenting or “juxtaphrenic peak” of the right hemidiaphragm, associated with elevation of the right hemidiaphragm
- On the lateral view, the atelectatic lobe will appear anteriorly and superiorly, behind the sternum
- It may not be visible on the lateral view because of overlying soft tissue
- The trachea may be shifted towards the right on the frontal view
- Occasionally, the right upper lobe will be completely collapsed and difficult to visualize on either frontal or lateral projections
- Secondary signs of atelectasis, as outlined above, may then be helpful
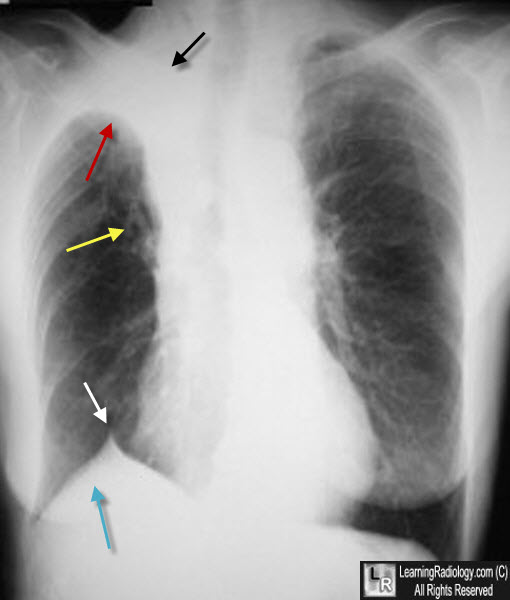
Atelectasis, Right Upper Lobe. There is a triangular or wedge-shaped density at the right apex (black arrow) that displaces the minor fissure upward (red arrow). The right hilum is elevated from volume loss (yellow arrow). There is a right juxtaphrenic peak (white arrow) of the right hemidiaphragm, which is also elevated in its entirety (blue arrow). The patient had a bronchogenic carcinoma obstructing the RUL bronchus.
The various faces of right upper lobe atelectasis. KR Kattan. Crit Rev Diagn Imaging. 1991:32 (2): 119-63
|
|
|
