|
|
Aspirated Foreign Body
General Considerations
- Children between 1-3 are most at risk
- Twice as common in males as females
- Up until age 15, both right and left main bronchi arise at about the same angle from the trachea so that objects may be aspirated into either side
- Afterwards, the right main bronchus arises in a less acute, more straight path than the left
- The most frequently aspirated foreign bodies are food (especially nuts), teeth, dental devices and medical instruments
- Some nuts, such as peanuts, have an oil that leads to inflammation and edema making them more difficult to expel
Clinical Findings
- Many go undiscovered delaying diagnosis
- Cough
- Wheeze
- Stridor
- Dyspnea
- Cyanosis
- Asphyxia if the object obstructs he trachea or larynx
Imaging Findings
- A normal chest radiograph does not exclude an aspirated foreign body
- Children will more often display signs of air-trapping while adults will more often show atelectasis
- 80% of aspirated foreign bodies will be non-opaque on conventional radiography
- Hyperinflation of one lung or lobe may occur (obstructive emphysema)
- Lobar or segmental atelectasis
- Mediastinal shift
- Pneumomediastinum
- Confirmatory imaging studies
- If the patient is clinically able, an expiratory chest radiograph may demonstrate air-trapping on the affected side by lack of collapse of the lung and shift of the mediastinum away from the side with the foreign body
- If the patient is a child or otherwise not able to cooperate for an expiratory study, a decubitus view of the chest, with the suspected side down, may show a lack of collapse of the air-trapped lung
- CT may demonstrate the foreign body or better show the narrowing of the bronchus
Differential Diagnosis
- Asthma
- In an adult, a large pulmonary embolus may appear to cause increased lucency of one hemithorax
- Swyer-James syndrome
- Lack of soft tissue on one side, such as from a mastectomy or Poland Syndrome
Treatment
Complications
- Look for lead lines. Any child who ingests a foreign body may have Pica.
- Mediastinitis or tracheoesophageal fistulas
- Air trapping leading
- Obstructive emphysema
- Atelectasis
- Post-obstructive pneumonia
- Abscess
- Bronchiectasis
Prognosis
- Prognosis is excellent if the foreign body is removed expeditiously (within 24 hours)


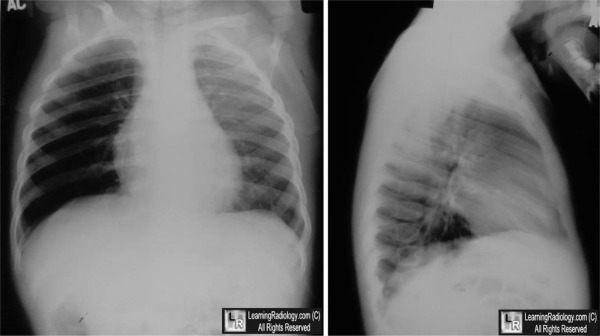
Aspirated Foreign Body (peanut). Upper photo: There is unilateral increased lucency of the entire right hemithorax (white arrow).
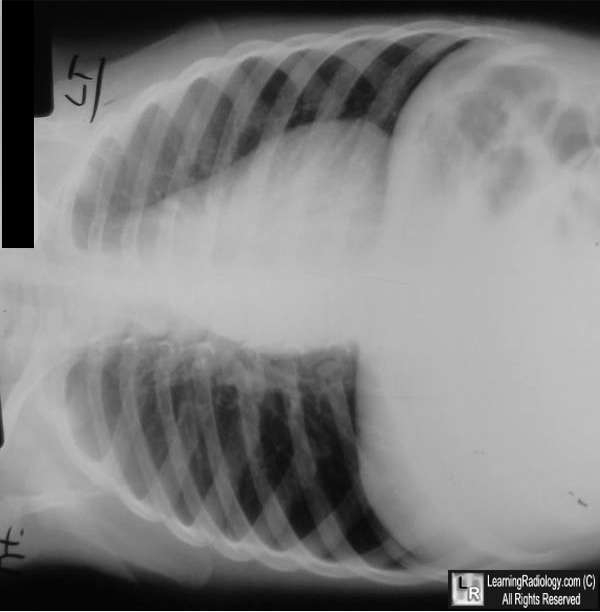
There is no shift of the heart. The right hemidiaphragm is in normal position Lower photo: A right-side down decubitus view of the chest, here shown as it was obtained, fails to show the expected normal collapse of the right lung in this position. This supports the presence of air-trapping in the right lung due to a non-opaque foreign body--in this case, a peanut in the right main bronchus
For this same photo without the arrows, click here and here
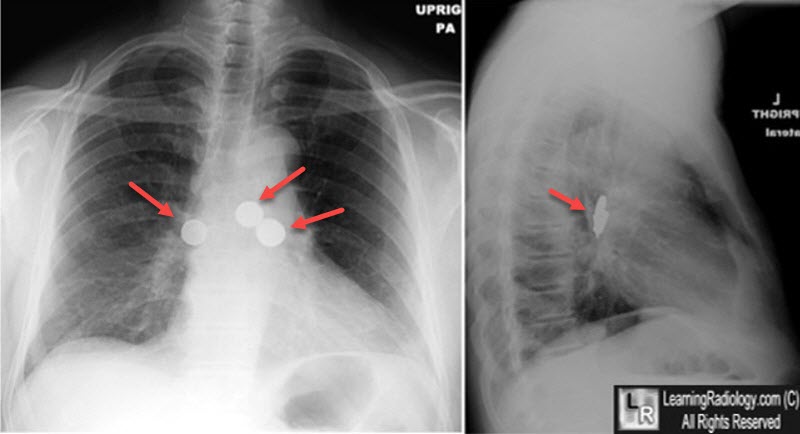
Aspirated Foreign Bodies (Coins). There are several (three in all) coins that were aspirated and are now lodged in the right and left main bronchi (red arrows).
For more information, click on the link if you see this icon 
Foreign Body Aspiration. ME Warshawsky. eMedicine.
The lateral decubitus film. An aid in determining air-trapping in children. MA Capitanio MA and JA Kirkpatrick. Radiology. May 1972;103(2):460-2
|
|
|

{kind=link}
{kind=link}