|
|
Fat Embolism
General Considerations
- Occurs in a high percentage of cases with major trauma (90%) but only rarely to clinical fat embolism syndrome (FES) which includes triad of findings in:
- Skin - petechiae
- Brain – cerebral dysfunction
- Lung – respiratory failure
- Fat emboli are known to lead to an inflammatory response
- Fat emboli may pass through a patent foramen ovale in 20-30% of patients to reach the systemic circulation
- Besides trauma, fat embolism may be seen in acute pancreatitis, burns, joint surgery, liposuction and cardiopulmonary bypass
Clinical Findings
- Diagnosis is based mainly on clinical findings beginning 24-72 hours after trauma, surgery or long bone fracture
- Dyspnea
- Petechiae
- Cognitive dysfunction
Imaging Findings
- Diffuse bilateral airspace disease about 24-48 hours after clinical onset
- On CT, nodular or ground-glass opacities may be seen
- Otherwise, the findings may be similar to lung contusions or ARDS
- Fractures of the femur, pelvis and tibia are most common
Differential Diagnosis
- Acute respiratory distress syndrome
- Pulmonary embolism
Treatment
- Methylprednisolone, when given prophylactically, may be helpful
- Supportive care
- Oxygen
- Hydration
- Blood replacement
Prognosis
- Mortality can be 10% even in those diagnosed earlier
- Pulmonary sequelae may take a year to resolve
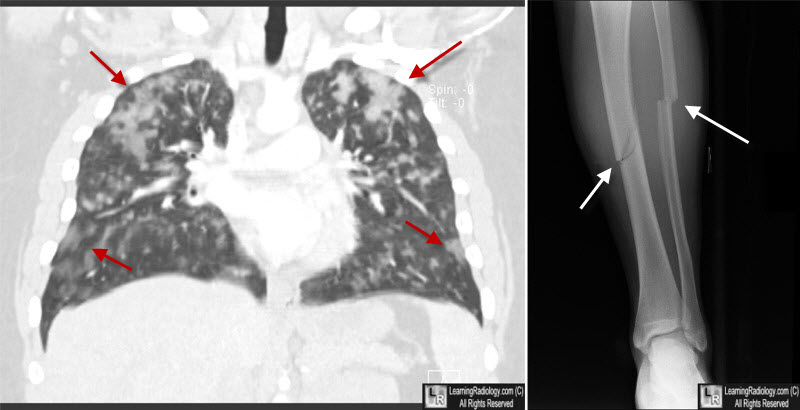
Fat Embolism. CT at left shows multiple nodular densities and patchy airspace disease scattered throughout both lungs (red arrows). The radiograph at right in the same patient shows fractures of both the tibia and fibula (white arrows).
Fat Embolism. eMedicine. CS Bulauitan and R Gupta.
Emergency management of fat embolism syndrome. N Shaikh. J Emerg Trauma Shock. 2009 Jan-Apr; 2(1): 29–33.
|
|
|
