|
|
Developmental Dislocation/Dysplasia of the Hip
Congenital Hip Dislocation, Dysplasia, DDH
General Considerations
- Also called congenital hip dislocation/dysplasia
- It may be associated with ligamentous laxity of the hip, but this is not likely to be the sole reason for its occurrence
Associations
- Higher prevalence in Native Americans and Laplanders
- Lower prevalence in Chinese and black populations
- 10X more frequent in children whose parents had DDH
- 80% females
- More common in first-born child
- More common with breech presentations
- More common in the left hip than right
- Oligohydramnios occurs more frequently
- It is bilateral in about 20% of cases
Clinical Findings
- Earliest signs can be seen in newborn
- Ortalani click – is more of a clunk when the when the hip reduces into the acetabulum, with the hip in abduction
- Galeazzi sign – at 3-6 months, dislocated leg appears shorter than the other with the child supine with knees flexed
- Bilateral dislocations may manifest with a waddling gait
Imaging Findings
- Ultrasound may be performed with measurement of the alpha angle (greater than 60degress considered normal) and beta angle (less than 55 degrees considered normal)
- Conventional radiography – using a standing or supine AP view of the pelvis
- The following illustration and description of the measurements comes from Medscape (see citation below)
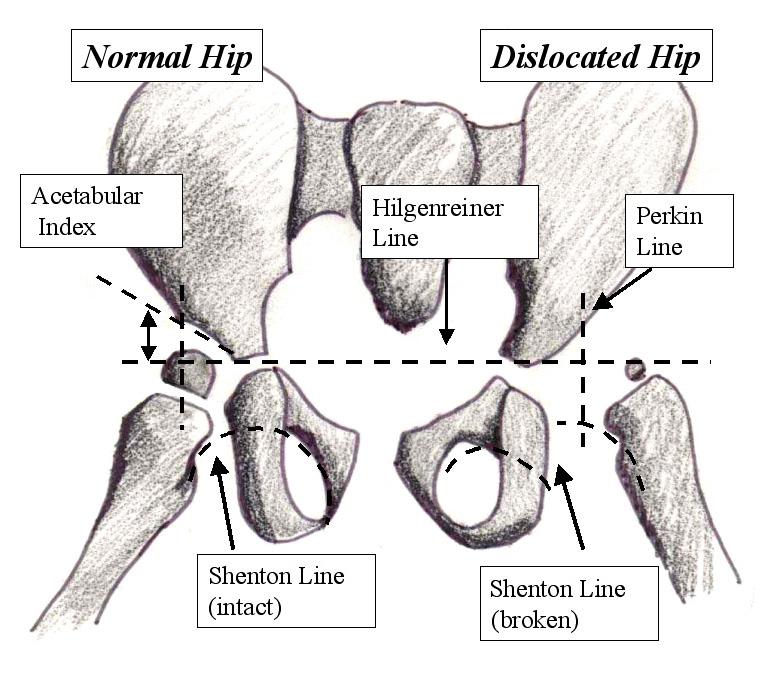 Illustration and caption From eMedicine Illustration and caption From eMedicine
Typical radiographic evaluation of developmental dysplasia of hip (DDH). From anteroposterior radiograph of hips, horizontal line (Hilgenreiner line) is drawn between each triradiate cartilage. Next, lines are drawn perpendicular to Hilgenreiner line through superolateral edge of acetabulum (Perkin line), dividing hip into 4 quadrants. Proximal medial femur should be in lower medial quadrant, or ossific nucleus of femoral head, if present (usually observed in patients aged 4-7 months), should be in lower medial quadrant. Acetabular index is angle between Hilgenreiner line and line drawn from triradiate cartilage to lateral edge of acetabulum. Typically, this angle decreases with age and should measure less than 20° by 2 years of age. Shenton line is drawn from medial aspect of femoral neck to inferior border of pubic rami. It should create smooth arc that is not disrupted. Disruption of Shenton line indicates presence of some degree of hip subluxation
- Three-dimensional reconstructions showing the anatomy of the hip joint and shape of the acetabulum can be helpful
Differential Diagnosis
Treatment
- Children younger than 6 months with instability upon examination are treated with a form of bracing
- If not effective or child older than 6 months, closed reduction may be performed
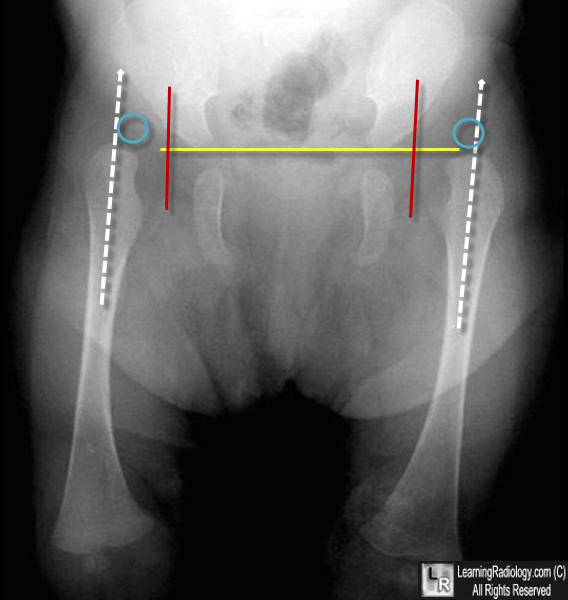
Bilateral Hip Dislocation. The yellow line is the Hilgenreiner line. The two vertical lines (red) are Perkins' lines. The capital femoral epiphysis (blue circles), not yet ossified, should normally lie in the lower inner quadrant formed by the intersections of Hilgenreiner's and Perkins' lines. It falls in the outer quadrants for both hips. Both are dislocated. A straight line drawn through the shaft of the femur (dashed white line) usually intersects some part of the acetabulum normally. Here, neither does. If drawn, Shenton's lines would be "broken" on both sides.
Developmental Dysplasia of the Hip. Junichi Tamai and James J McCarthy. eMedicine.
|
|
|
