|
|
Duodenal Diverticulum
General Considerations
- Relatively common (up to 6% of upper GI examinations) in adults
- Usually arise in 2nd portion of the duodenum (85%) within 1-2 cm of the ampulla of Vater
- Like almost all GI diverticula, they are false diverticula with herniation of the mucosa and submucosa through the muscular layer
- Usually single but may be multiple
- Peak incidence in 5th-6th decade
- Usually asymptomatic
- Duodenum is second most common site of diverticula formation in GI tract after colon
Clinical Findings
- 90-95% are asymptomatic
- Symptoms are usually from associated complications – pain and bleeding
Imaging Findings
- Vary in size from mm to several centimeters
- Arise from medial wall (mesenteric side) of duodenal sweep most commonly
- Most are juxta-ampullary
- Mushroom shape with narrow neck and broad base
- May have an air-fluid level if large enough on upright studies
Differential Diagnosis
- Intraluminal diverticulum – are congenital, have a “wind sock”-like structure filled with barium and are surrounded by a radiolucent halo
Treatment
- No treatment unless causing complications
- Surgery may be indicated in cases of hemorrhage or perforation
Complications
- GI bleed
- Perforation
- Pancreatobiliary disease, e.g., cholelithiasis and pancreatitis

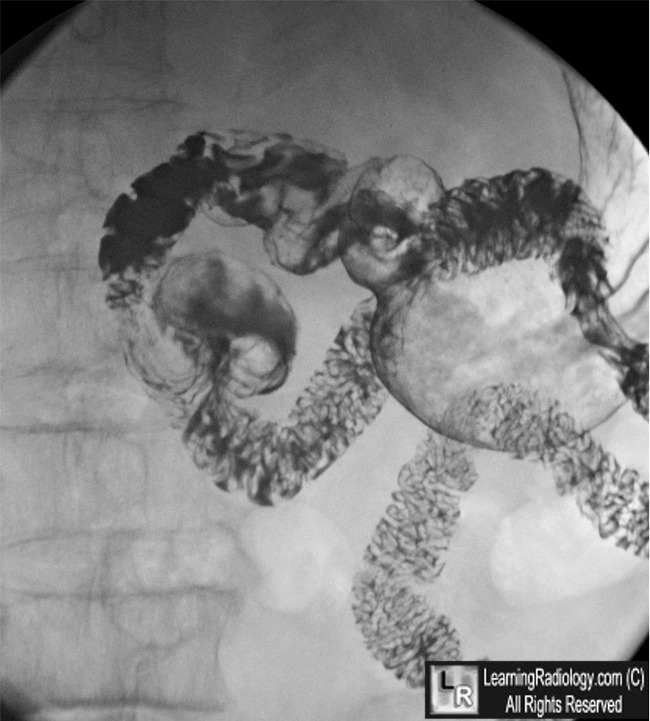
Duodenal Diverticulum. There is a large air and contrast filled diverticulum (yellow arrow) arising off of the medial wall of the 2nd portion of the duodenum, near the ampulla (white arrow). The stomach (S), duodenal bulb (B), duodenum (D) and jejunum (J) are also outlined.
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}