|
|
Superior Mesenteric Artery Syndrome
- Compression of 3rd portion of
duodenum between the aorta and superior mesenteric
artery (SMA)
- Females more affected than males
- Most often in older children,
adolescents
- Some doubt the true existence of
the syndrome
- Pathophysiology
- Narrowing of angle between SMA
and aorta
- SMA usually forms an angle
of 45 degrees with the aorta
- Etiologies
- Prolonged bed rest in supine
position (body cast, whole-body burns, surgery)
- Substantial and, frequently,
rapid weight loss
- Anorexia nervosa or
malnutrition
- Loss of abdominal muscle tone
(as in pregnancy)
- May be congenital
- Seen in those with asthenic
build
- Exaggerated lumbar lordosis
- Clinical findings
- Epigastric pain
- Nausea
- Repetitive vomiting
- Abdominal cramping
- Typically findings are worst
in supine position and may be relived by changing to
the prone or left lateral decubitus positions
- Associated with a higher than
normal incidence of peptic ulcer disease and hyperchlorhydria
- Imaging findings
- Usually requires upper GI or
CT of abdomen for diagnosis
- Megaduodenum
- Pronounced dilatation of 1st and 2nd portion of duodenum and frequently stomach
- Best seen in supine position
- Compression of duodenum
between aorta and SMA
- Vertical linear compression
defect in transverse portion of duodenum overlying
spine
- Abrupt change in caliber distal
to compression defect
- Treatment
- Relief of compression by
postural change into prone knee-elbow position
- Weight gain
- Surgery is indicated only when
conservative treatment is not successful
- Duodenojejunostomy is the most frequently used procedure
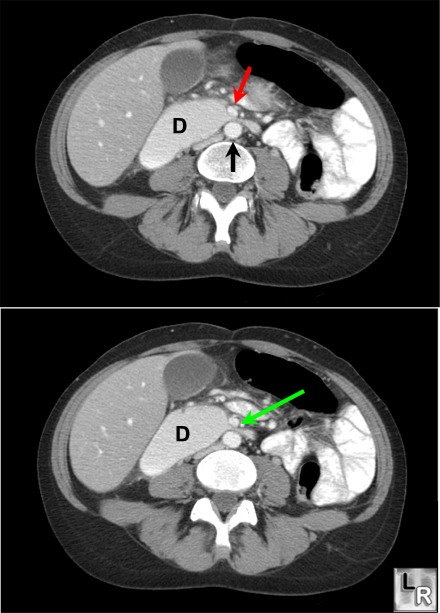
Superior Mesenteric Artery Syndrome. Axial CT scans of the upper abdomen
show a dilated 2nd portion of the duodenum (D)
just proximal to a narrowed segment of the 3rd portion
of the duodenum (green arrow) compressed between the superior mesenteric artery (red
arrow) and the aorta (black arrow)
Dahnert, 5th Edition
Avinash Shetty, MD and Ivor D Hill, MB, ChB, DCH, FCP, MD: eMedicine
|
|
|
