|
|
Wilm's Tumor
Nephroblastoma
General Considerations
- Most common abdominal malignancy of children
- Both kidneys affected synchronously or metachronously in 5-10%
- Peak incidence at 2.5-3 years
- More common in blacks than whites with an approximately equal gender distribution
Clinical Findings
- Asymptomatic abdominal mass most common
- Abdominal pain
- Hematuria
- Hypertension
- Urinary tract infection
- Varicocele
- Aniridia
- Hemihypertrophy
- Beckwith-Wiedemann Syndrome
Imaging Findings
- Ultrasound is frequently the first study
- CT is useful in determining extent, lymph nodes and liver metastases
- Tumors tend to be large and may cross midline
- Sharply marginated possibly with compressed normal renal tissue
- May be partially cystic from necrosis
- Curvilinear or punctate calcifications
- Invasion of IVC by tumor
- Hypervascular tumors
- On MRI, tumor tends to have decreased signal on T1 and increased on T2
Differential Diagnosis
- Neuroblastoma
- Polycystic kidney disease
- Rhabdomyosarcoma
Treatment
- Nephrectomy followed by chemotherapy
- Postoperative radiation therapy for stage II and IV lesions
Complications
- Impaired renal function following nephrectomy is rare
- Chemotherapeutic agents may be hepatotoxic
- Scoliosis following radiation therapy
Prognosis


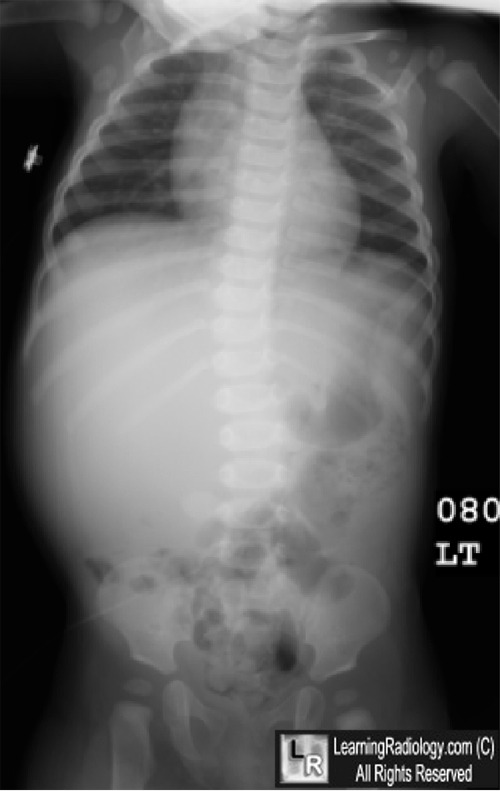
Wilm's Tumor. Conventional radiograph of abdomen shows a large right upper mass displacing
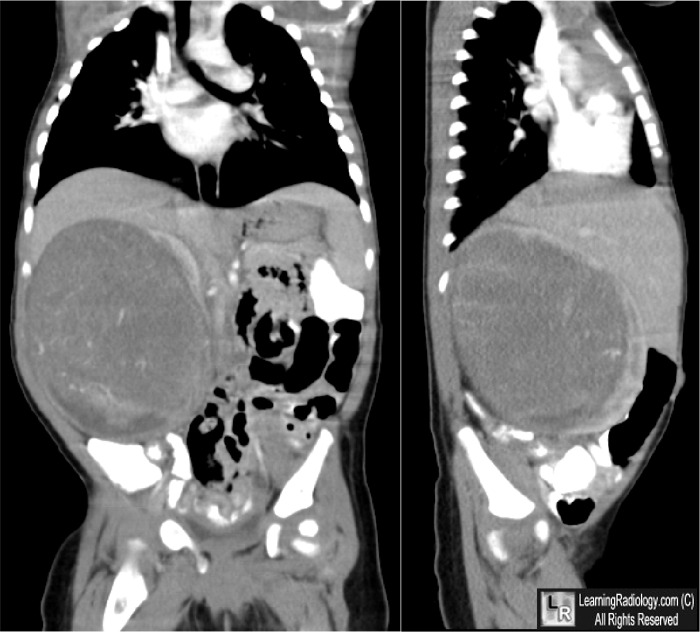
bowel loops into the pelvis and across the midline (blue arrows). Coronal and sagittal reformatted CT
demonstrate a large, heterogeneous mass arising from the right kidney (white arrows). A small
sliver of functioning right kidney is seen to enhance (yellow arrow).
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here and here
|
|
|

{kind=link}
{kind=link}