|
|
Renal Infarction
General Considerations
- Thrombotic disease usually affects larger vessels
- Includes main renal artery
- Patients with thrombotic disease usually present with hypertension or renal insufficiency
- Usually results from atherosclerosis
- But, blunt abdominal trauma may cause intimal tears with subsequent dissection and thrombosis
- Emboli can affect vessels of various sizes depending on the size of the emboli
- Renal artery emboli usually come from cardiac source
- Embolic disease usually produces acute symptoms
- Sudden onset of flank pain
- Hematuria
- Proteinuria
- Fever
- Leukocytosis
Causes
- Trauma
- Blunt abdominal trauma
- Traumatic avulsion of renal artery
- Surgery
- Embolism
- Cardiac origin
- Rheumatic heart disease with arrhythmia
- Myocardial infarction
- Prosthetic valves
- Myocardial trauma
- Left atrial or mural thrombus
- Myocardial tumors
- Subacute bacterial endocarditis
- Catheters
- Angiographic catheter manipulation
- Umbilical artery catheter above level of renal arteries
- Arterial thrombosis
- Arteriosclerosis
- Thromboangiitis obliterans
- Polyarteritis nodosa
- Syphilitic cardiovascular disease
- Aneurysms of the aorta or renal artery
- Sickle cell disease
- Sudden complete renal vein thrombosis
Lobar Renal Infarction
- Early signs
- Focal attenuation of collecting system
- Focally absent nephrogram
- Triangular with base at cortex
- Late signs
- Normal or small kidney(s)
- Focally atrophied parenchyma with normal interpapillary line
- Cortical atrophy and irregular scarring are seen as late sequelae
- CT
- Subtle renal infarcts are best demonstrated on CT
- Appear as wedge-shaped, cortically based, hypodense areas
- Triangular in shape with widest part at the cortex (base of infarct)
- Non-perfused area corresponding to vascular division
- Renal swelling may also be seen
- Cortical rim sign
- Entire kidney is nonenhancing except for the outer 24 mm of cortex, which are perfused by capsular branches
- US
- Focally increased echogenicity
- Color flow Doppler aids in diagnosis of renal artery thrombosis
- There is absence of an intrarenal arterial signal
- Tardus parvus waveform is seen if incomplete occlusion or collateral supply
- Nuclear medicine
- Nuclear imaging shows a photopenic area corresponding to the region of ischemia or infarction
Chronic Renal Infarction
- Pathology
- All elements of kidney atrophied with replacement by interstitial fibrosis
- Normal or small kidney with smooth contour
- Globally atrophied parenchyma
- Diminished or absent contrast material density
- US
- Increased echogenicity (by 17 days)
- Angiography
- Normal intrarenal venous architecture
- Late visualization of renal arteries on abdominal aortogram
- Provides the definitive diagnosis
- Abrupt termination of vessels or filling defects
- With end-stage renal artery thrombosis
- Small kidney with smooth contour, unless multiple small infarcts have occurred independently
Treatment
- Anticoagulation
- Intra-arterial thrombolytic therapy
- Surgical revascularization
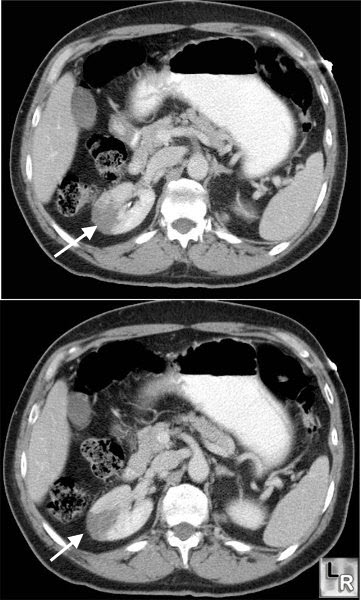
Renal Infarct. Two contrast-enhanced axial CT images demonstrate a
wedge-shaped
non-enhancing lesion in the right kidney with no perinephric
inflammatory stranding (white arrows).
Amersham
|
|
|
