|
|
Splenic Laceration
Submitted by David Allen, MD
- Most frequently injured solid parenchymal organ in
blunt trauma to the abdomen
- Splenic injury often associated with other organ
injuries
- 20% with left rib fractures
- 25% with left renal injury
- 40% with splenic laceration have rib fractures
- Subcapsular hematoma
- Crescentic low-attenuation area
- Usually along lateral margin
- Flattens normal convex margin of spleen
- Parenchymal lesion
- Indistinct splenic margin
- Inhomogeneous enhancement
- Fractured spleen
- Complete separation of fragments
- Intrasplenic hematoma
- Rounded mass
- Disrupted splenic capsule
- Often has associated hemoperitoneum
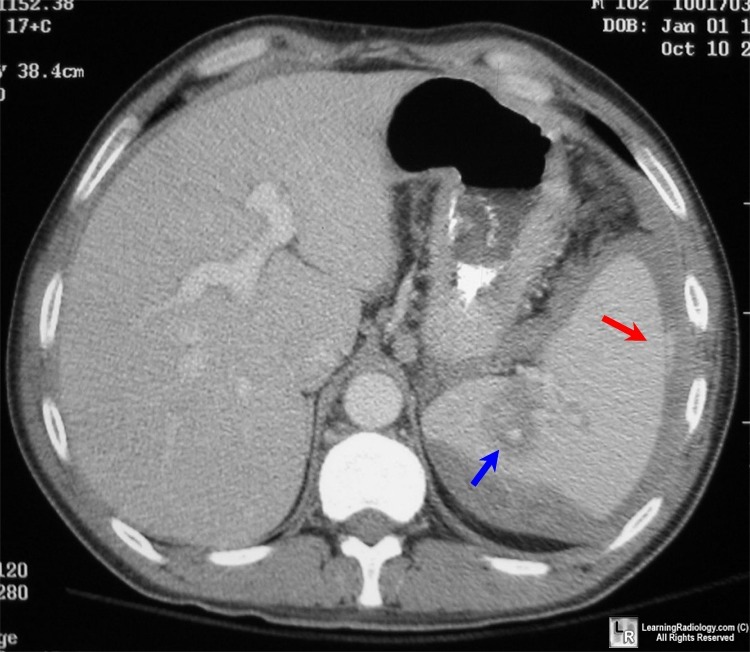
CT shows a subcapsular hematoma with a splenic laceration extending from the
capsule to the hilum with an intraparenchymal hematoma (blue arrow). Within the intraparenchymal and subcapsular
hematomas are areas of hyperdensity that represent active extravasation (red arrow).
- Pitfalls in diagnosis
- Normal lobulation or cleft mimics tear
- Adjacent unopacified bowel loop (jejunum) simulates
splenic tissue
- Scans taken too early after bolus
- Spleen can be inhomogeneous due to differential
enhancement of red and white pulp
- Previous infarct can mimic laceration
- Perisplenic fluid from ascites or lavage mimics
hemoperitoneum
- Grades of laceration
- Grade I: small laceration < 1cm and small
subcapsular hematoma
- Grade II: moderate laceration 1-3cm and moderate
subcapsular hematoma
- Grade III: large laceration > 3cm not involving
hilum with large subcapsular hematoma
- Grade IV: laceration involving the hilum
- Grade V: destroyed spleen
- If part of hematoma is isodense to arterial blood on
an enhanced CT there is active extravasation
- Treatment
- Follow clinically
- Arterial embolization/coiling
- Splenorrhaphy
- Splenectomy
- Treatment options
- The higher the grade the more likely the need for an
intervention
- Grade I and II are usually followed clinically
unless they worsen
- Grade IV and V usually require surgery
- 15% of low-grade lacerations develop a delayed
hemorrhage after 2 days
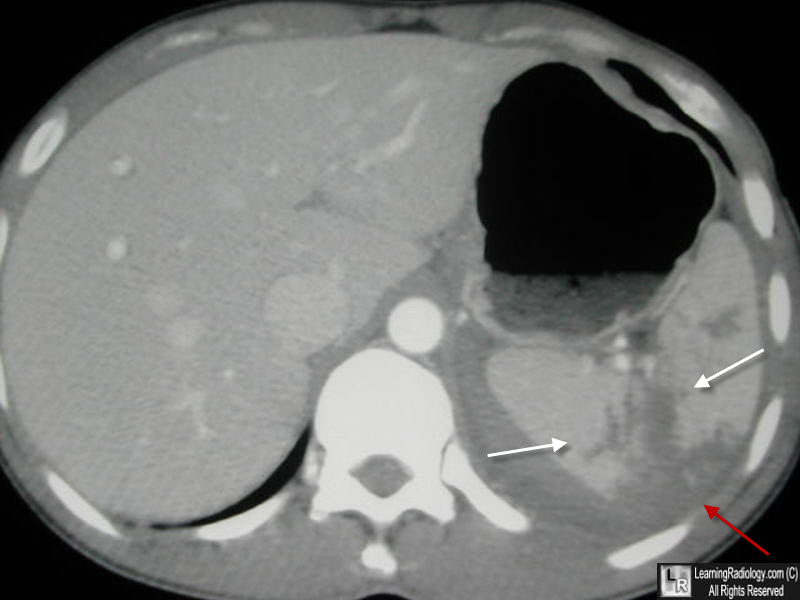
Splenic laceration. CT shows a subcapsular hematoma (red arrow) with a splenic laceration (white arrows).
|
|
|
