|
|
Hypertrophic Pyloric Stenosis
- Age
- Usually manifests at 2-8 weeks of life
- Clinical
- Nonbilious projectile vomiting with progression over a period of several weeks
after birth (15-20%)
- Palpable olive-shaped mass (80% sensitive in
experienced hands)
- Positive family history
- Nasogastric aspirate >10 ml
- UGI findings
- Pyloric wall thickness >10 mm
- Elongation and narrowing of pyloric canal (2-4
cm in length)
- "Double / triple track sign"
- Crowding of mucosal folds in pyloric channel
- "String sign"
- Passing of small barium streak through
pyloric channel
- Twining recess = "diamond sign"
- Transient triangular tent-like cleft / niche in midportion of pyloric canal with apex pointing inferiorly secondary to
mucosal bulging between two separated hypertrophied muscle bundles
on the greater curvature side within pyloric channel
- "Pyloric teat"
- Outpouching along lesser curvature due to
disruption of antral peristalsis
- "Antral beaking"
- Mass impression upon antrum with streak of
barium pointing toward pyloric channel
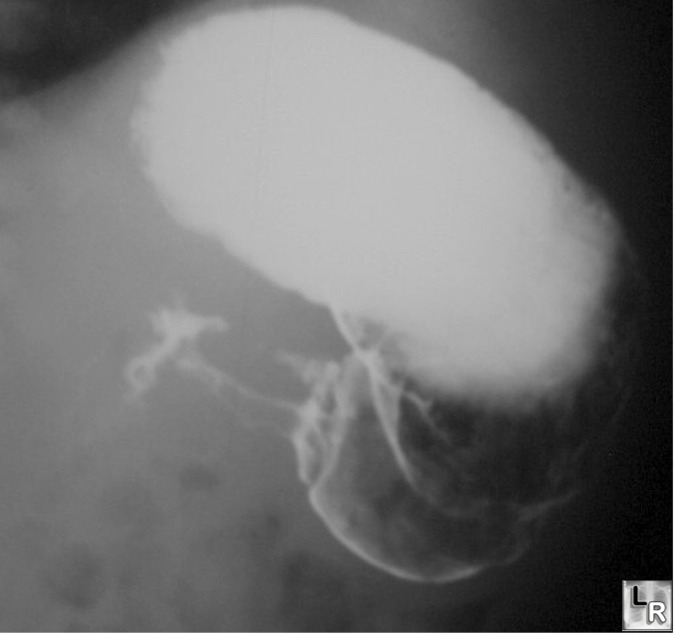
Stomach shows double tracking in region of pyloric
canal,
indentation on base of bulb and delayed gastric emptying
- Kirklin sign = "mushroom sign"
- Indentation of base of bulb (in 50%)
- Gastric distension with fluid
- Active gastric hyperperistalsis
- "Caterpillar sign"
- Gastric hyperperistaltic waves
- US findings
- "Target sign"
- Hypoechoic ring of hypertrophied pyloric
muscle around echogenic mucosa centrally on cross-section
- "Cervix sign"
- Indentation of muscle mass on fluid-filled
antrum on longitudinal section
- "Antral nipple sign"
- Redundant pyloric channel mucosa protruding
into gastric antrum
- Pyloric volume >1.4 cm3 (= 1/4 ÷ x [maximum
pyloric diameter]2 x pyloric length)
- Most criteria independent of contracted or
relaxed state
- Pyloric length (mm) + 3.64 x muscle thickness
(mm) > 25
- Pyloric muscle wall thickness >3 mm
- Pyloric transverse diameter >13 mm with
pyloric channel closed
- Elongated pyloric canal >17 mm in length
- Exaggerated peristaltic waves
- Delayed gastric emptying of fluid into
duodenum
- Complications
- Hypochloremic metabolic alkalosis
- DDx
- Infantile pylorospasm
- Muscle thickness between 1.5 and 3 mm
- Variable caliber of antral narrowing
- Antral peristalsis
- Delayed gastric emptying
- Elongation of pylorus
- Prognosis
- Resolves in several days / ? early stage of evolving pyloric
stenosis
- Treatment
- Effective with metoclopramide
hydrochloride
- Milk allergy
- Eosinophilic gastroenteritis
|
|
|
