|
Hiatal Hernia
· Two main types: sliding and paraesophageal
· Most are acquired
· Incidence increases with age
· About 1/5 of patients with a hiatal hernia, usually the sliding type, have associated gastro-esophageal reflux (GERD)
Sliding Hiatal Hernia (99%)
· Most hiatal hernias are asymptomatic
· There is an association between the presence of some hiatal hernias and clinically significant gastroesophageal reflux (GERD)
o Gastro-esophageal reflux also occurs in patients without any visible hiatal hernia
§ Usually due to dysfunction of lower esophageal sphincter which normally acts to prevent gastric acid from repeatedly refluxing into esophagus
· Radiologic findings of hiatal hernia
o Bulbous area of distal esophagus containing contrast at level of diaphragm with failure of esophagus to narrow on multiple images as it passes through esophageal hiatus
§ Distalmost esophagus should not measure more than 50% of diameter of the tubular esophagus
o Extension of multiple gastric mucosal folds above the diaphragm
o Sometimes, a thin, circumferential filling-defect in the distal esophagus called a Schatzki’s Ring may be visible
§ Schatzki’s ring marks position of esophagogastric junction so that its visualization above diaphragm defines the presence of a sliding hiatal hernia
· Some limit use of the term Schatzki’s ring to only those esophageal rings associated with dysphagia
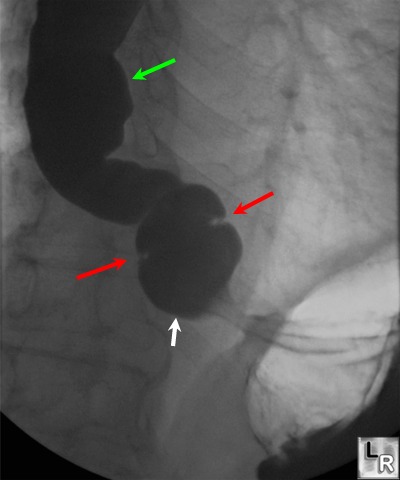
Hiatal Hernia with Schatzki's Ring. The red arrows point to a slit-like indentation which marks the
position of the esophago-gastric junction and, since it is seen above the diaphragm, therefore defines the presence of a hiatal hernia of the so-called sliding type. This indentation is called a Schatzki's ring (or "B ring") although that term is reserved by some only for such rings that produce dysphagia. The white arrow points to the herniated stomach while the green arrow points to disordered tertiary waves of contraction.
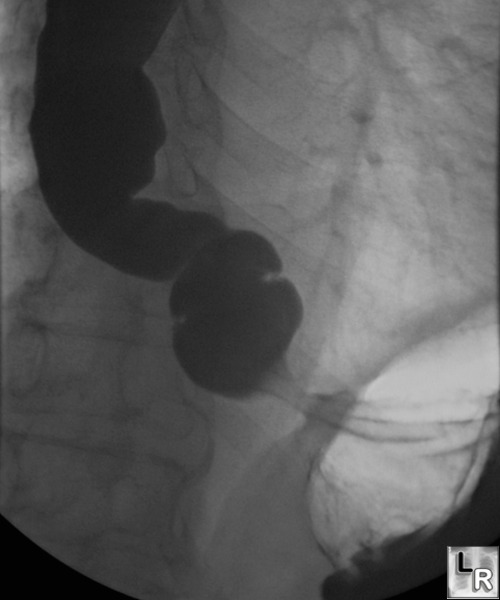
For a photo of the same image without arrows, click on this link
Complications
§ Large incarcerated hiatal hernias may slowly weep blood so that patients present with iron deficiency anemia, rather than reflux symptoms
§ Peptic esophagitis from reflux
§ Discrete marginal ulcers
§ Strictures
o The terminology can be confusing
§ Hiatal hernias, like any other hernias, may be reducible or incarcerated
§ Sliding refers to a hiatal hernia in which the EG junction is above the diaphragm, not to its reducibility
· A sliding hiatal hernia can be reducible or incarcerated
Paraesophageal Hiatal Hernia
· Portion of stomach herniates through esophageal hiatus and comes to lie above diaphragm but EG junction continues to be subdiaphragmatic
· Usually incarcerated
· Not associated with GE reflux
Intrathoracic stomach
· Cardia may still be subdiaphragmatic
· Greater curvature may be on left or right side
Congenitally short esophagus (rare)
· Gastric ectopy by reason of lack of lengthening of esophagus
· Short, straight esophagus
· Stomach in thorax
· Frequently associated with ulcer at EG junction
· GE reflux
Antireflux mechanisms
o Normally, the EG junction, the “A” or contractile ring above it and, lastly, the cricopharyngeous muscle
o Abnormally
§ Large, incarcerated hiatal hernias tend not to be associated with reflux
§ Paraesophageal hiatal hernias are usually not associated with reflux
Relationship between hiatal hernia and Barrett’s esophagus
o Barrett’s esophagus consists of columnar epithelium lining the esophagus
o Acquired condition related to chronic gastroesophageal reflux
§ An associated hiatal hernia is common
o Patients with a Barrett’s esophagus can develop
§ Ulcer
§ Stricture
§ Malignancy
· Patients with Barrett’s esophagus have a 30-40 times higher risk of esophageal adenocarcinoma than the general population
| 
{kind=link}