|
|
Emphysematous Cholecystitis
- General considerations
- Acute infection of gallbladder caused by gas-forming organism
- In about 1/3 = clostridium perfringens
- Also E. Coli and Klebsiella
- Rare – only 1% of all cases of acute cholecystitis
- Occurs more often in men
- As opposed to gallbladder disease in general which occurs more often in women
- Mostly are elderly patients (>60) with diabetes
- Vascular compromise of the cystic artery may play a role in the etiology
- Gallstones may be associated with the disease but are not thought to cause it
- Gas may occur in the wall and/or the lumen
- May spread to pericholecystic tissue
- Rarely, gas may escape into the bile ducts
- This is rare since cystic duct is usually occluded in cholecystitis
- Clinical findings
- As with cholecystitis, right upper quadrant (RUQ) pain and tenderness
- Leukocytosis
- Jaundice is rare
- Imaging findings
- Conventional radiography
- May show air in the wall or lumen of the gallbladder
- Air-fluid levels in the gallbladder will only be seen with images obtained with a horizontal beam, not on supine radiographs
- Gas may spread to the pericholecystic tissues
- These findings, if present on the conventional radiograph, usually herald a poor outcome from late-stage disease
- US findings
- Indistinct shadowing emanating from wall or lumen of gallbladder
- “Ring-down effect” or “comet tail” from shadowing from air in gallbladder lumen
- CT findings of cholecystitis
- Air in gallbladder wall is diagnostic of this disease
- Most common signs of non-emphysematous cholecystitis are gallbladder wall thickening >3mm, and
- Cholelithiasis
- Increased density of bile (>20 H)
- Loss of clear definition of gallbladder wall
- Pericholecystic fluid such as a halo of edema
- Treatment
- Definitive care involves surgical intervention
- Preoperative percutaneous drainage may improve survival
- Emergency cholecystectomy
- Complications
- Fivefold increase in perforation over uncomplicated acute cholecystitis
- Perforation of the gallbladder
- Frequency is declining because of earlier diagnosis of acute cholecystitis
- Diagnosis
- Pre-perforation conventional radiograph showing stones clustered in gallbladder may subsequently show stones scattered in RUQ after perforation
- Pericholecystic fluid collection on CT or US (not-specific)
- Scintography may show radiotracer outside of gallbladder in Morrison’s pouch or flank
- Treatment
- Preoperative percutaneous drainage of gallbladder and biloma
- Emergency surgery

Emphysematous Cholecystitis. Supine view of the abdomen shows air in the wall (blue arrows) of the gallbladder (GB). There is also a lucency within the lumen of the gallbladder (GB) suggesting air inside the lumen. There is no air-fluid level visible because this radiograph is obtained supine with a vertical x-ray beam. Just superior to the gallbladder is another collection of air (red arrow) that represents a pericholecystic abscess. The yellow arrow points to the end of a PEG tube in the stomach.
For this same photo without the arrows, click here
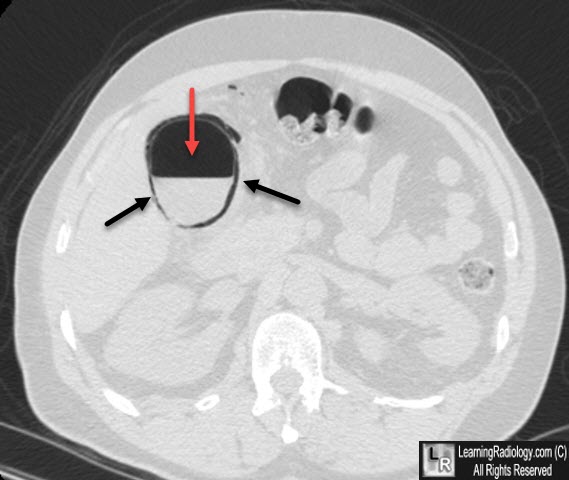
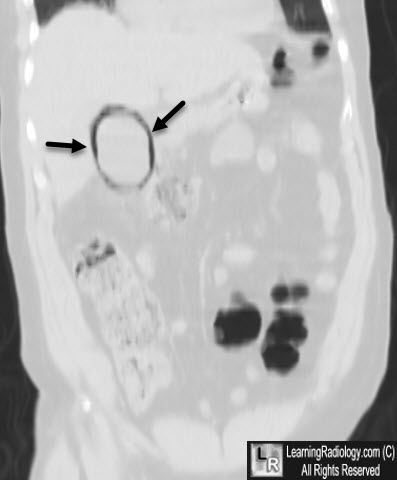
Emphysematous Cholecystitis. Air is contained both within the gallbladder lumen (see red arrow on upper axial image) and the wall of the gallbladder (black arrows on both the axial and lower coronal image).
Gore, R. and Levine, M: textbook of Gastrointestinal; Radiology, W.B. Saunders, 2000.
Moss, A., Gamsu, G. and Genant, H.: Computed Tomography of the Body. W.B. Saunders,1992.
|
|
|

{kind=link}
{kind=link}