|
|
Diverticulitis
Diverticulosis
General Considerations
- Herniation of mucosa and submucosa through muscular layers–pseudodiverticulum=false diverticulum=pulsion type
- Diverticula are reducible; they may be seen on one but not another BE
- Only proven association is with Marfan’s syndrome (20% get diverticulitis)
Location
- Almost always involves sigmoid; never rectum; more common on left
- In about 17%, the tics cover the entire colon
- In another 12%, they are isolated to right colon
Prediverticular Disease
- Saw-tooth appearance to the colon, usually sigmoid, with shortening of bowel, crowding of haustra and picket-fencing of folds
- Muscle spasm is present-may be relieved with glucagon
- Controversial as to whether this form can be symptomatic, i.e. pain
Diverticulosis
- May be due to low roughage, high refined-fiber diet
- More common in industrialized nations
- Arise between the mesenteric and anti-mesenteric teniae of the colon and project between circular muscle rings–not through them
- May vary in size from tiny projections to several cm in size
- Have variable filling
- Associated spasm and numerous tics in sigmoid may make it impossible to see polyp in this region–even difficult with colonoscopy
- On AC BE tics have sharp outer and fuzzy inner margins viewed en-face
- Giant sigmoid diverticulum–huge gas-containing cyst-like structure arising in left iliac fossa
Diverticulitis
- Perforation of diverticulum with pericolic abscess of varying size; not simply inflammation of a tic
Clinical Findings
- Pain and tenderness, mass in LLQ
- Fever, leukocytosis
Imaging Findings
CT
- Infiltration of pericolonic fat
- Bowel wall thickening >1cm
- Abscess
- Fluid or free air in peritoneal cavity
- Colovesical or colovaginal fistula
- Intramural sinus tracts
BE
- Extraluminal contrast
- Pericolonic abscess produces mass effect
- Double-tracking=barium in longitudinal sinus tract in wall
- Spasm is an indirect sign of diverticulitis
- Fistula to bladder (diverticulitis is most common cause of non-traumatic fistula here) or small bowel or vagina (diverticulitis causes 1/3 of fistulae to vagina)
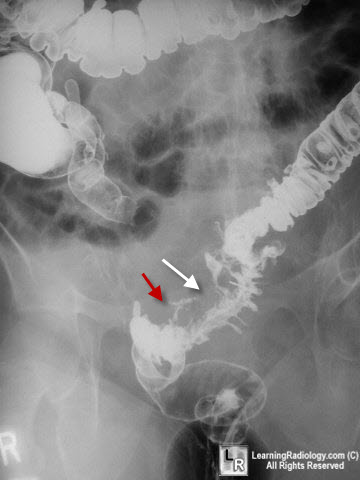
Diverticulitis, Barium Enema. There is an abscess in the left lower quadrant which is producing compression on the barium-filled sigmoid (red arrow), and there is evidence of extraluminal contrast (red arrow) from a perforated diverticulum,
Conventional Radiography
- Sentinel loop or, less likely, LBO
- Air bubbles in abscess
- Pneumoperitoneum (rare)
Differential Diagnosis
- Colon ca-but mucosa is left intact in diverticulitis
- Crohn’s disease-may be indistinguishable if TI not involved in Crohn’s
- Ischemic colitis–only if sigmoid is involved
- Radiation colitis
Complications
- Peritonitis–usually the perforation is walled off but it may spread throughout the peritoneal cavity or the retroperitoneum
- If a ruptured diverticulum is a strong clinical consideration prior to contrast study, water soluble contrast should be used rather than barium
- Obstruction–is rare
- Bleeding–see below
Hemorrhage from Diverticulosis
- Does't involve Diverticulitis
- 75% of those that bleed are in right colon
- Clinically, massive rectal hemorrhage without pain
- May be diagnosed with nuclear med bleeding scan or angiography
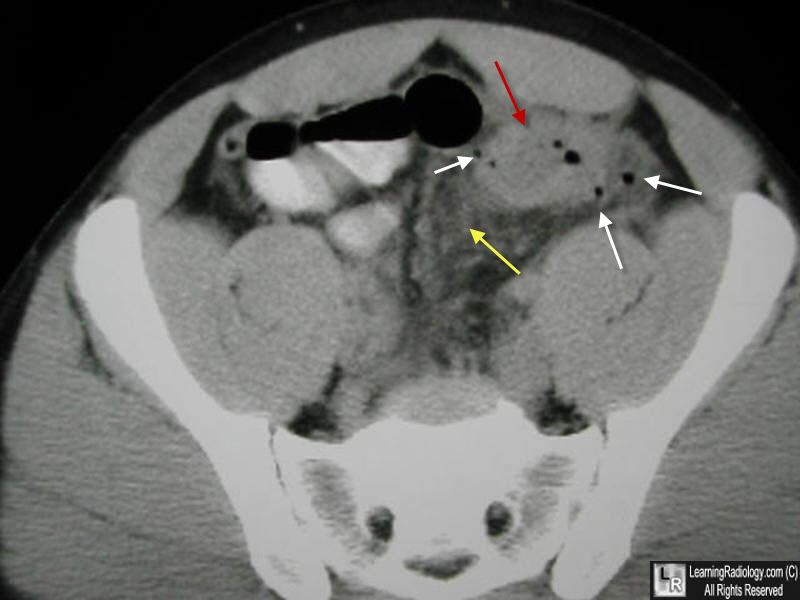
Diverticulitis. There is an abscess in the left lower quadrant (red arrow), with thickening of the bowel wall, infiltration of the pericolonic fat (yellow arrow) and multiple areas of extraluminal air.
|
|
|
