|
|
Tracheal Stenosis
General Considerations
- Ulceration of the mucosa and inflammation with granulation tissue formation produce the stenosis
- Most occur at the site of the cuff, next most at the site of the stoma (in a tracheostomy) and least at the site of the tip of the tube
- Causes include
- Trauma, as in prolonged endotracheal intubation
- Inflammatory disease like sarcoid and polychondritis
- Neoplasm
- Collagen vascular disease
Clinical Findings
Imaging Findings
- Conventional AP and lateral views are often obtained preliminarily
- CT will demonstrate the lesion, especially on coronal reconstructions
- The tracheal wall is normally 1-2 mm thick
- Concentric or eccentric narrowing of the trachea, usually 1.5 to 2.5 cm in length
- Granulation soft tissue will be seen internal to the cartilaginous structures
- Cotton-Myer Classification system
Classification |
From |
To |
Grade I |
No obstruction |
50% obstruction |
Grade II |
51% obstruction |
70% obstruction |
Grade III |
71% obstruction |
99% obstruction |
Grade IV |
No detectable lumen |
Treatment
- Use of low-pressure cuffs has almost eliminated prolonged intubation as a cause
- Treatment could include long-term tracheostomy, long-term intraluminal stent or surgical repair, either externally or endoscopically
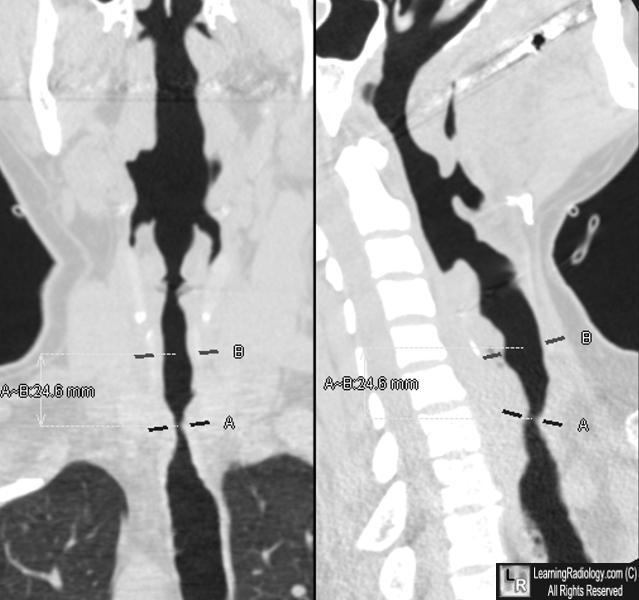
Tracheal Stenosis. Coronal and sagittal MPR images demonstrate marked narrowing of the trachea at point A and slightly less narrow extending to point B. The patient had a history of long-term endotracheal use.
Tracheal Stenosis after Tracheostomy or Intubation: Review with Special Regard to Cause and Management. A Sarper, A Ayten, I Eser, O Ozbudak, and A Demircan. Tex Heart Inst J. 2005; 32(2): 154–158.
Using CT to Diagnose Nonneoplastic Tracheal Abnormalities Appearance of the Tracheal Wall. EM Webb, BM Elicker and WR Webb. May 2000, Volume 174, Number 5
|
|
|
