|
|
Reexpansion Pulmonary Edema
General Considerations
- Rare complication of rapid expansion of the lung passively collapsed by a large pleural effusion or pneumothorax
- Greatest risks are in young patients with large pneumothoraces, pulmonary collapse of more than 7 days, or removal of up to 3 liters of pleural fluid at one time
- But it has been reported to occur with as little as 1 liter of fluid removed
- Pathophysiology not known
Clinical Findings
- About 2/3 of patients are symptomatic during the first hour after intervention
- Remainder develop signs and symptoms by 24 hours
- Cough
- Rapidly progressing tachypnea and dyspnea
- Tachycardia
- Hypoxemia
Imaging Findings
- Unilateral airspace opacities in the involved lung within 2-4 hours usually lasting 2 (but up to 7) days before reverting to normal
- The opposite lung is very rarely involved; thus it is unilateral airspace disease resembling pulmonary edema
- Effusion is uncommon
- CT shows ground-glass opacities, septal thickening, consolidation
Differential Diagnosis
Treatment
- Conservative and supportive (oxygen)
- Intubation is usually not needed
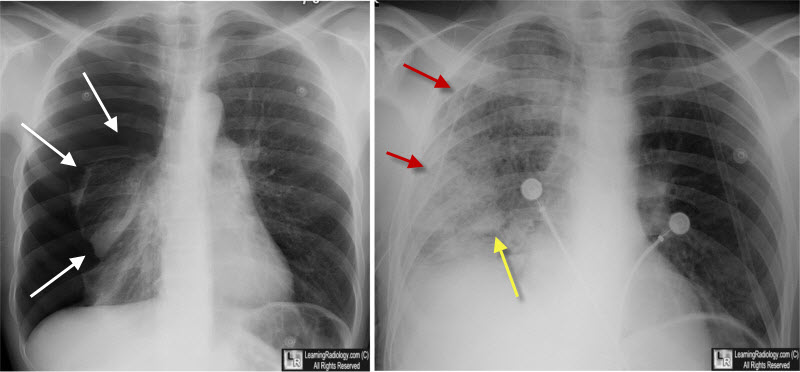
Reexpansion Pulmonary Edema. On the left, there is a large right-sided pneumothorax (white arrows). An hour after chest tube insertion (red arrows), there is now airspace disease in the right lung (yellow arrow), which has been reexpanded.
Mingolla GP. Reexpansion pulmonary edema. J Emerg Med. 2009;36:80–2
Reexpansion pulmonary edema after therapeutic thoracentesis. Olívia Meira Dias, Lisete Ribeiro Teixeira, and Francisco S Vargas. Clinics (Sao Paulo). 2010 Dec; 65(12): 1387–1389.
Reexpansion pulmonary edema after chest drainage for pneumothorax: A case report and literature overview. M. Verhagen, J.M. van Buijtenen, L.M.G. Geeraedts Jr. Respiratory Medicine Case Reports, Volume 14, 2015, Pages 10–12
|
|
|
