|
|
Pneumocystis Carinii Pneumonia
Pneumocystis Jerovecii
General Considerations
- Most common cause of interstitial pneumonia in immunocompromised patients
- Organism
- Protozoan / fungus Pneumocystis carinii (jiroveci)
Predisposed
- AIDS
- Debilitated
- Premature infants
- Children with hypogammaglobulinemia
- Other immunocompromised patients
- Congenital immunodeficiency syndromes
- Lymphoproliferative disorders
- Organ transplant recipients
- Patients on long-term corticosteroid therapy
- Patients on chemotherapy for cancer
Associated infections
- CMV
- Mycobacterium avium-intracellulare (MAI)
- Herpes simplex
Clinical Findings
- Severe dyspnea and cyanosis
- Subacute insidious onset of malaise and slight cough (frequent in AIDS patients)
- Respiratory failure
- WBC slightly elevated (polys)
- Lymphopenia (50%) indicates poor prognosis
Imaging findings
- Normal CXR in 10-40%
- Bilateral diffuse symmetric finely granular / reticular interstitial / airspace infiltrates in 80%
- Characteristic central location
- Rapid progression to diffuse airspace disease
- Resembles non-cardiogenic pulmonary edema
- Pleural effusion and hilar lymphadenopathy are uncommon
- Isolated lobar disease / focal parenchymal opacities
- Lung nodules ± cavitation
- Hilar / mediastinal lymphadenopathy
- Thin- / thick-walled cysts
- Cavities with predilection for upper lobes
CT Findings
- Patchwork pattern (56%)
- Bilateral, asymmetric patchy mosaic appearance
- Ground-glass pattern (26%)
- Bilateral, diffuse air-space disease in symmetric distribution
- Interstitial pattern (18%)
- Bilateral, symmetric / asymmetric, reticular markings (thickening of lobular septa)
- Abnormal air-filled spaces (38%)
- Pneumatocoeles
- Thin-walled spaces without lobar predilection resolving within 6 months
- Subpleural bullae due to emphysema
- Thin-walled cysts
- Necrosis of pneumocystis granuloma
- Pneumothorax (13%)
- Lymphadenopathy (18%)
- Pleural effusion (18%)
Pulmonary nodules and cavities
- Usually due to malignancy
- Leukemia, lymphoma
- Kaposi sarcoma
- Metastasis
- Or septic emboli
- Pulmonary cavities usually due to superimposed fungal / mycobacterial infection
Nuclear medicine
- Bilateral and diffuse Ga-67 uptake without mediastinal involvement prior to roentgenographic changes
Course
- Usually responds to therapy in 5-7 days
- Effect of prophylactic use of aerosolized pentamidine
- Redistribution of infection to upper lobes
Complications
- Cystic lung disease
- Central location to cysts
- Spontaneous pneumothorax, frequently bilateral (6-7%)
- Disseminated extrapulmonary disease (1%)
- Punctate / rimlike calcifications within enlarged lymph nodes and abdominal viscera
DDx
- Non-cardiogenic pulmonary edema
- TB
- MAI infection
Diagnosis
- Sputum collection
- Bronchoscopy with lavage
- Transbronchial or transthoracic or open lung Bx

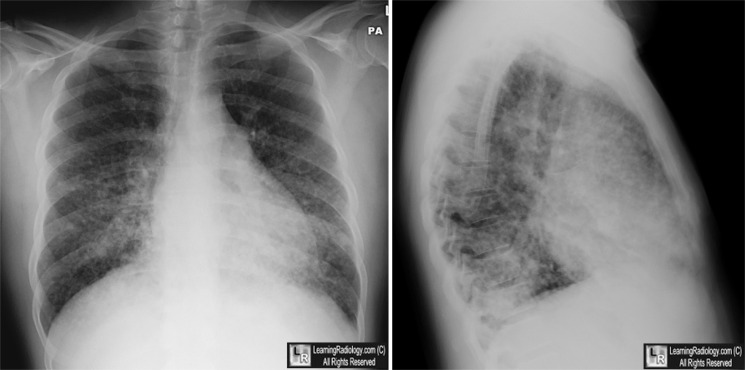
Pneumocystis Pneumonia. There is diffuse, mostly reticular, interstitial lung disease greater at the bases. is a similar picture to that of congestive heart failure under other clinical circumstances.
For these same photos without the arrows, click here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}