|
|
Lymphangitic Carcinomatosis
Lymphangitic Spread of Tumor
- Pulmonary nodules are the most common expression of metastatic disease in the lungs
- Such tumor emboli are spread hematogenously
- In lymphangitic carcinomatosis tumor grows in and obstructs lymphatics in the lung producing a pattern that is radiologically similar to pulmonary interstitial edema from heart failure including
- Kerley B lines
- Thickening of the fissures
- Pleural effusions, especially laminar effusion
- The findings may be unilateral, which should alert you to the possibility of lymphangitic spread rather than congestive heart failure
- Focal unilateral disease accounts for 50% of cases.
- This pattern is found especially with underlying bronchogenic carcinoma
- The most common primary malignancies to produce lymphangitic spread are adenocarcinomas
- Most common primary sites are
- Breast
- Lungs
- Stomach
- Pancreas
- Cervix
- Larynx
- Colon
- Lymphangitic carcinomatosis is believed to initially occur as hematogenous spread of tumor to the lungs
- The tumor then invades the vessels wall and into the lymphatics
- Tumor spreads through the lymphatics which provide little resistance to spread
- Alternatively, there may be central obstruction of mediastinal or hilar lymph nodes leading to direct infiltration
- Most common presenting complaint is breathlessness
- Other symptoms may include dry cough or hemoptysis
- Symptoms will often occur before the onset of any radiographic abnormality
- The study done first is usually conventional chest radiography
- Sensitivity of chest radiography in the detection of lymphangitic carcinomatosis is only approximately 25%
- CT findings
- Irregular, nodular, and/or smooth interlobular septal thickening
- Thickening of the fissures from infiltration of lymphatics in the subpleural space
- Peribronchovascular thickening which predominates over interlobular septal thickening in a minority of patients
- Polygonal arcades or polygons with prominence of the centrilobular bronchovascular bundle in association with interlobular septal thickening (50%)
- Mediastinal and/or hilar lymphadenopathy (30-50%)
- Pleural effusions (30-50%)
- Laminar pleural effusions are common
- Nodular opacities1
- Sarcoidosis
- Silicosis
- Coal worker's pneumoconiosis
- Extrinsic allergic alveolitis (hypersensitivity pneumonitis)
- Unilateral pulmonary edema
- Lymphoma and Kaposi sarcoma
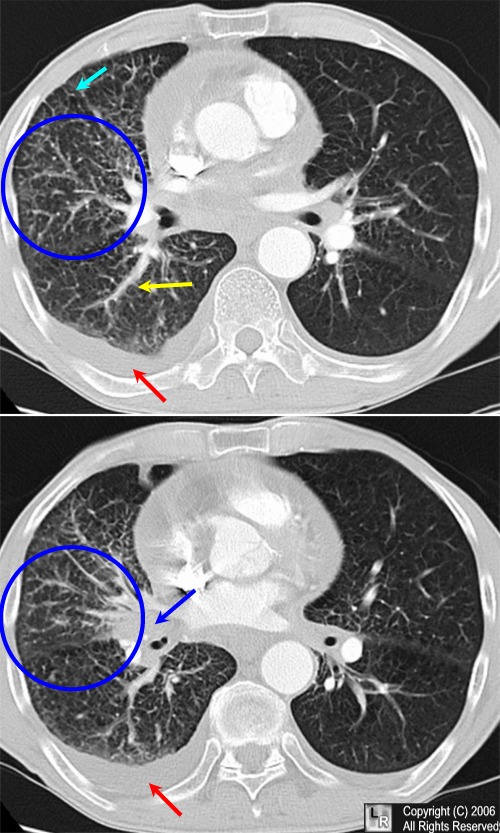
Lymphangitic carcinomatosis. A central bronchogenic carcinoma (blue arrow) is producing
unilateral interstitial edema (blue circles) characteristic of lymphangitic carcinomatosis with a pleural effusion
(red arrow), thickening and irregularity of the bronchovascular bundles (yellow arrow)
and thickening of the interlobular septa (light blue arrow).
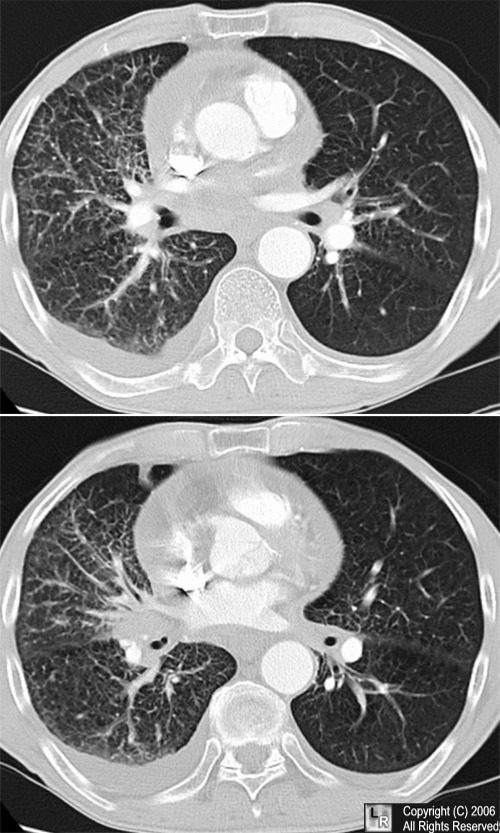
For the same photo without the arrows, click here
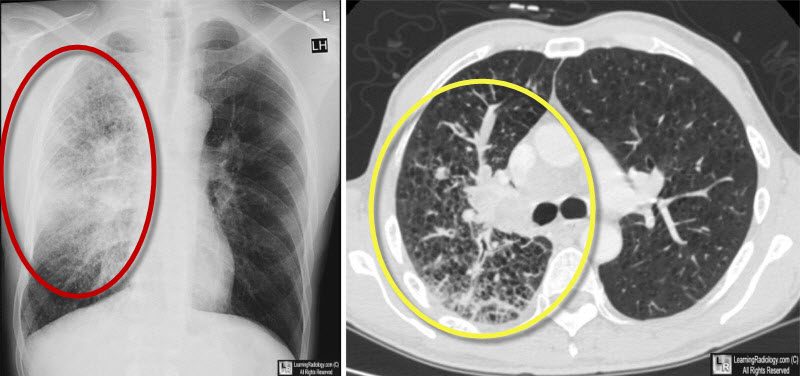
Lymphangitic carcinomatosis. Chest radiograph on left shows unilateral interstitial lung disease, primarily in the upper lung field (red oval). CT scan of the chest reveals the same interstitial prominence with septal lines and perivascular nodularity eminating from a central right hilar mass (yellow oval).
|
|
|

{kind=link}