|
|
Bronchiectasis
General Considerations
- Pathologic dilation of the proximal and medium sized airways from weakening or destruction of their walls
- Three major causes are: obstruction, infection and traction, the most common being infectious
- Bronchiectasis may occur when there is prolonged partial obstruction, e.g. slow- growing neoplasms, foreign bodies
- Infection produces bronchial wall obstruction and is most important cause of bronchiectasis
- Traction comes from a force, usually due to increased elastic recoil in the surrounding lung, which pulls the bronchus and dilates it such as sarcoid in the upper lobes and chronic interstitial lung diseases in the lower lobes
- Bronchi are inflamed, collapse easily and produce air-flow obstruction
- Most often involves a lobe or segment
Clinical Findings
- Classical clinical triad: chronic cough, excess sputum production and repeated infection
- Hemoptysis
- Shortness of breath
- Wheezing
- Fever is rare even with infection
Imaging Findings
- Location
- Proximal, frequently upper lobe, bronchiectasis is characteristic of allergic bronchopulmonary aspergillosis (ABPA)
- Bronchiectasis from viral or pyogenic infections is usually at the bases
- Tuberculous bronchiectasis is usually at the apices
- Diffuse bronchiectasis
- Impaired mucus clearing e.g. cystic fibrosis and Kartagener
- Chronic diffuse airways disease (chronic bronchitis, asthma, bronchiolitis obliterans
- Immune deficiency states
- CT is the study of choice with a sensitivity of up to 97% and a specificity up to 99%
- Signet ring appearance on CT : normally, the vessel is larger than the corresponding bronchus
- In bronchiectasis, the bronchus is larger than the corresponding vessel
- “Tramlines” or “honeycombing” represents dilated, thickened bronchial walls
- Volume loss due to destruction of lung tissue
- Multiple small nodular densities from plugged alveoli
- Lack of normal, bronchial tapering
- Non uniform bronchial dilation
- Cystic lesions, often with air-fluid levels, and frequently in a cluster
- Bronchial wall thickening
- Types
Types of Bronchiectasis |
Types |
Description |
Cylindrical |
Dilated bronchi with straight and usually regular outlines; tram-track lines parallel to each other; signet ring appearance when seen in axial plane |
Saccular or cystic |
Ballooned appearance of bronchi may have air-fluid levels; large, cystic areas with a honeycomb appearance; thicker than bullae of emphysema |
Varicose |
Bronchi with dilated segments and other areas of constriction; beaded bronchi |
Differential Diagnosis
- Proximal bronchiectasis is characteristic of allergic bronchopulmonary aspergillosis (ABPA)
- Mycobacterium avium complex (MAC) infection may occur with HIV or in women, especially, over the age of 60 and may produce bronchiectasis
- Alpha-1 antitrypsin deficiency
- Cystic fibrosis
- Emphysema
- TB
Treatment
- Antibiotics
- Chest physiotherapy
- Surgery
Complications
- Pneumonia
- Empyema
- Lung abscess
- Cor pulmonale
- Pneumothorax
Prognosis
- Prognosis is good and depends more on the predisposing condition


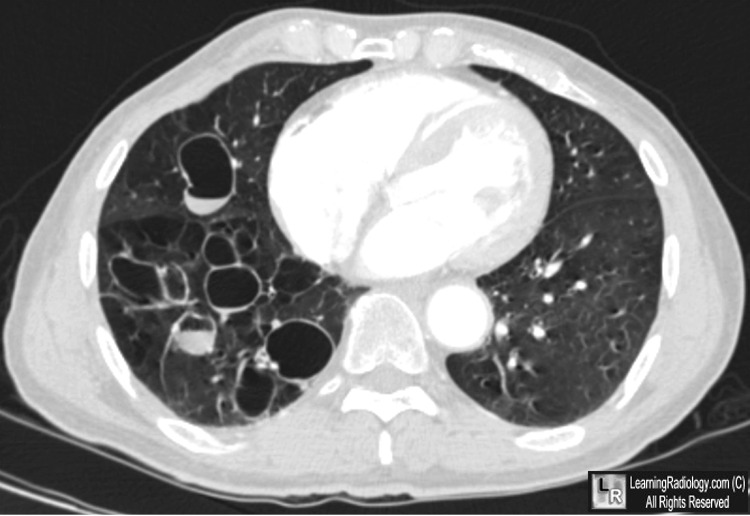
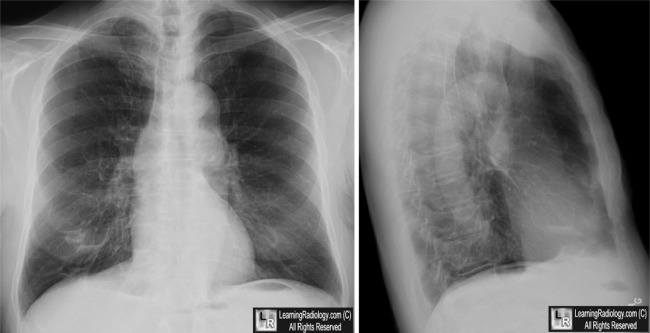
Cystic Bronchiectasis. CT: Markedly dilated bronchi are seen, some with air-fluid levels (yellow arrows), mostly in the right lung. Chest radiographs: Demonstrate thin-walled, cystic structures in right lower lobe (white arrow), some with air-fluid levels (yellow arrows).
For these same photos without the arrows, click here and here
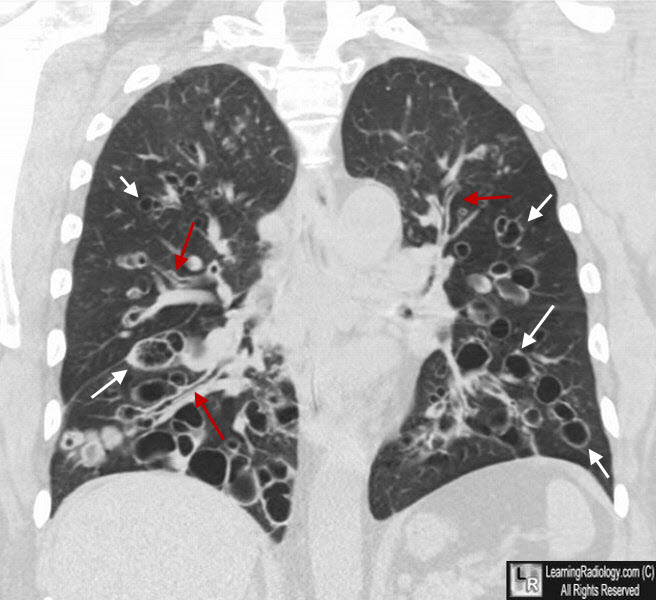
Cystic Bronchiectasis. Coronal CT again shows markedly dilated bronchi (white arrows point to several). The red arrows point to the"tramlines" of bronchiectasis.
For more information, click on the link if you see this icon 
Bronchiectasis. eMedicine. EE Emmons, I Hassan.
|
|
|

{kind=link}
{kind=link}