|
|
Aortic Arch Anomalies
Right, double, cervical aortic arch
Right Aortic Arch
General
- Most are asymptomatic
- Unless they cause encircling vascular ring like pulmonary sling
- Can be complex lesions requiring multiple projections
Left Aortic Arch With Anomalous Right Subclavian Artery (RSCA)
- Occurs in less than 1% of people
- RSCA passes posterior to esophagus
- Pushes trachea and esophagus forward
- Produces oblique shadow above aortic arch on frontal film
- Origin of RSCA may be dilated
- Diverticulum of Kommerell is most commonly seen with a right aortic arch and anomalous left subclavian artery (LSCA)
Right Aortic Arch
- Types
- At least five different types
- Only two of importance
- Mirror Image Type — Type I
- Aberrant left subclavian — Type II
General considerations
- Recognized by leftward displacement of barium-filled esophagus
- Of air-filled trachea
- Aortic knob is absent from left side
- Aorta descends on right
- Para-aortic stripe returns to left side of spine just above diaphragm
- Mirror-image type almost always has associated congenital heart disease (CHD)
- Usually Tetralogy of Fallot
- Aberrant Left Subclavian type rarely has associated CHD
- Most common variety of right arch
Type 1—Mirror Image Type
- Secondary to interruption of left arch just distal to ductus arteriosis
- Associated with congenital heart disease 98% of time
- Imaging Findings
- No posterior impression on trachea or barium-filled esophagus
- Heart is usually abnormal in size or shape
- Aorta descends on right
Type ll—Aberrant Left Subclavian
- Secondary to interruption of left aortic arch between LCC and LSC arteries
- Associated with cardiac defects 5-10% of the time
- Tetralogy of Fallot most often (71%)
- ASD or VSD next most often (21%)
- Coarctation of aorta rarely (7%)
- Anomalous left subclavian artery (retroesophageal and retrotracheal)
- Aorta descends on right
- Imaging Findings Right Aortic Arch with Aberrant LSCA
- Posterior impression on trachea and barium-filled esophagus
- Heart is usually normal in size and shape
- Aorta descends on right
- If there is a mirror-image right aortic arch, then
- 90% will have Tetralogy of Fallot
- 6% with Truncus Arteriosis
- 5% with Tricuspid Atresia
- If the person has the following lesions, then the association with a mirror-image arch is
- Truncus arteriosis 33%
- Tetralogy of Fallot 25%
- Transposition 10%
- Tricuspid atresia 5%
- VSD 2%
Double Aortic Arch
General considerations
- Most common vascular ring
- Rarely associated with congenital heart disease
- Vascular ring produces tracheal and/or esophageal compression
- Caused by persistence of R and L IV branchial arches
- Passes on both sides of trachea
- Joins posteriorly behind esophagus
- Right arch is larger and higher
- Left arch is smaller and lower
- Barium swallow shows bilateral impressions on frontal view
- Posterior impression on lateral view
- Angiogram is characteristic
- Clinical
- Symptoms may begin at birth and include
- Tracheal compression, or
- Difficulty swallowing
- Anatomy
- Right arch supplies RSCA and RCC
- Left arch supplies LCC and LSCA
- Double Aortic Arch Imaging Findings
- Right arch is higher and larger
- Left arch is lower and smaller
- Produces reverse S on esophagram on AP
- On lateral, arches are posterior to esophagus and anterior to trachea
Cervical Aortic Arch
- General
- Rare
- Usually asymptomatic
- May present as pulsating supraclavicular mass
- May produce vascular ring and compress airway
- Embryogenesis uncertain
- Over 80% are right-sided
- Imaging Findings–Right-sided lesions
- Right-sided cervical aortic arches
- Right apical mass-like density
- Absence of aortic knob on left
- Aorta descends on the left
- Displace the trachea and esophagus forward
- Branching may be normal or mirror-image
- Imaging Findings–Left-sided lesions
- Left-sided cervical aortic arches
- Aortic knob at apex of lung
- Descend on the left
- Do not displace the trachea or esophagus forward
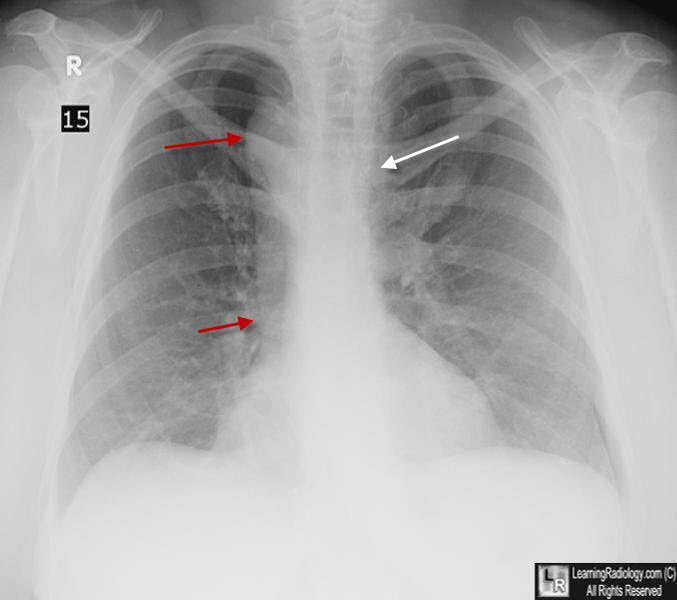
Right Aortic Arch. The aortic knob is not visible in its normal position on the left (white arrow). The knob and descending thoracic aorta are seen on the right (red arrows). This patient did not have congenital heart disease.
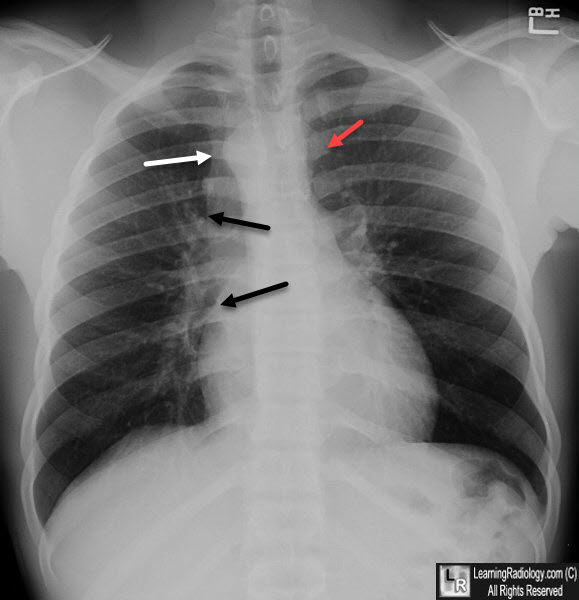
Right Aortic Arch. The aortic knob is not visible in its normal position on the left (redarrow). The knob (white arrow) and descending thoracic aorta (black arrows) are seen on the right. This patient did not have congenital heart disease.
|
|
|
