
RecognizingCongestiveHeart Failure
© William Herring, MD, FACR
Congestive Heart FailureX-ray patterns
Pulmonary Interstitial Edema
Pulmonary Alveolar Edema
Congestive Heart Failure Four Signs of Pulmonary interstitial edema
Thickening of the interlobular septa
Kerley B lines
Peribronchial cuffing
Wall is normally hairline thin
Thickening of the fissures
Fluid in the subpleural space incontinuity with interlobular septa
Pleural effusions
Normal
5-10 mm Hg
Cephalization
10-15 mm
Kerley B Lines
15-20
Pulmonary Interstitial Edema
20-25
Pulmonary Alveolar Edema
> 25
Left Atrial PressuresCorrelated With Pathologic Findings
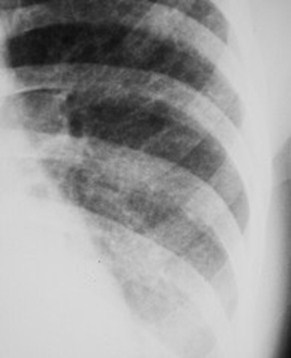
Kerley B Lines
B=distended interlobular septa
Location and appearance
Bases
1-2 cm long
Horizontal in direction
Perpendicular to pleural surface
Multiple Kerley B lines atthe left lung base
These are faint whitelines perpendicular tothe pleural surface and1-2cm long
Kerley A and C Lines
A=connective tissue near bronchoarterialbundle distends with fluid
Location and appearance
Near hilum
Run obliquely
Longer than B lines
C=reticular network of lines
C Lines probably don’t exist
Intersectingnetwork of linesare Kerley A linesin proper clinicalsetting
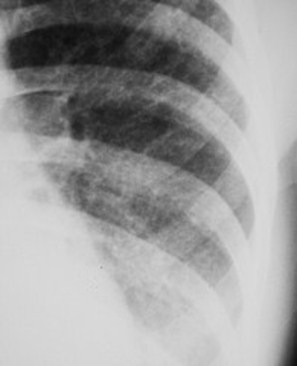
Peribronchial Cuffing
Bronchial wall usually not visible
Interstitial fluid accumulates around bronchi
Causes thickening of bronchial wall
When seen on end, looks like little “doughnuts”
Only meaningful when seen distal to hilar area;peribronchial cuffing may be normal in hila
Numerous small circular“doughnuts” seen inlung represent fluid inbronchial walls whenseen in conjunction withother signs of CHF
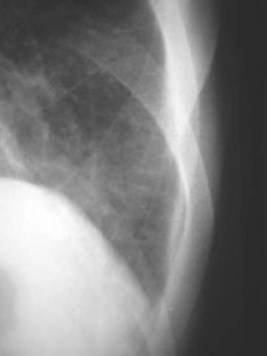
Fluid in The Fissures
Fluid collects in the subpleural space
Between visceral pleura and lungparenchyma
Normal fissure is thickness of asharpened pencil line
Fluid may collect in any fissure
Major, minor, accessory fissures, azygousfissure
Fluid in the minor fissure
Fissures may be seennormally but are usuallyno thicker than the pointof a sharpened pencil
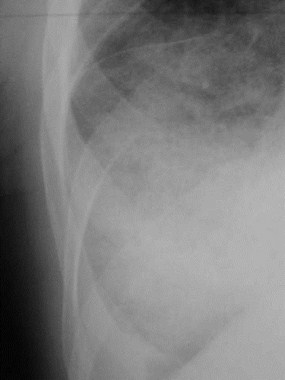
Pleural Effusion
Either in the pleural space or subpleural inlocation
Laminar effusions collect beneath visceralpleura (subpleural)
In loose connective tissue between lung andpleura
Same location as “pseudotumors”

Laminar effusion in CHF
A laminar effusionactually collects in theloose connective tissuejust inside the visceralpleura
Congestive Heart FailurePulmonary alveolar edema
Fluffy, indistinct patchy densities
Outer third of lung frequently spared
Bat-wing or butterfly configuration
Lower lung zones more affected thanupper
Pulmonary alveolaredema has a“butterfly” or “bat-wing” configuration

Pulmonary Alveolar EdemaClearing
Generally clears in 3 days or less
Resolution usually begins peripherallyand moves centrally
Pulmonary EdemaTypes
Cardiogenic
Neurogenic
Increased capillary permeability
E.g. Allergic reactions
Congestive Heart FailureCommon Causes of
Coronary artery disease
Hypertension
Cardiomyopathy
Valvular lesions
AS, MS
L to R shunts
Congestive Heart FailureClinical
Usually from left heart failure
Shortness of breath
Paroxysmal nocturnal dyspnea
Orthopnea
Cough
Right heart failure
Edema
Take Home Points
The four reliable signs of CHF are:
Kerley B lines
Fluid in the fissures
Peribronchial cuffing
Pleural effusion
NOT cardiomegaly
NOT cephalization

Which of the followingpatients has CHF?
Answer follows on slide after question
Quiz
Does this patient have CHF?
Answer follows on next slide
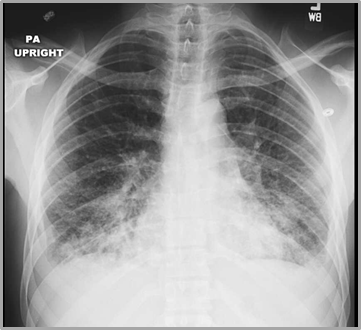
Yes, this is CHF
There are Blines at theright lung baseand a rightlaminareffusion
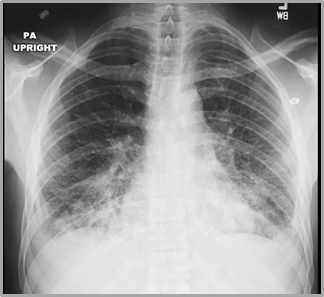
Does this patient have CHF?
Answer follows on next slide

Yes, this is CHF
There is diffuseairspace(alveolar) diseasewhich hassomewhat of a“bat-wing”appearancecharacteristic ofpulmonary edema
Answer follows on next slide
Does this patient have CHF?

No, this is not CHF
There are multiplenodules in both lungsfrom metastaticdisease
Answer follows on next slide
Does this patient have CHF?


There are Kerley B linesvisible at both lung bases
Yes, this is CHF
Continue
Congratulations, You Graduate

I knowCHFwhen Isee it
Want to learn more about CHF? Go to this linkWant to return to the beginning of this module? Click here