
The Fundamentals ofChest Roentgenology
The Fundamentals ofChest Roentgenology
© William Herring, MD, FACR
To exit, click back button on browser
To learn more . . .
To learn more about a topic click on theblue link wherever you see this icon

The Fundamentals of ChestRoentgenology
Fundamental Observations
Silhouette sign
Air bronchograms
Solid spheres vs. hollow tubes
Basic Disease Processes
Alveolar vs. interstitial lung disease
Opacified hemithorax
Cavities
The Fundamentals of ChestRoentgenology
Diseases
Congestive Heart Failure
Pneumothorax
When two objects of the samedensity touch each other, theedge between them disappearsWhen two objects of the samedensity touch each other, theedge between them disappears
A
B
Silhouette Sign
Using the Silhouette Sign
Right middle lobe silhouettes right heartborder
Lingula silhouettes left heart border
Right lower lobe silhouettes righthemidiaphragm
Left lower lobe silhouettes lefthemidiaphragm

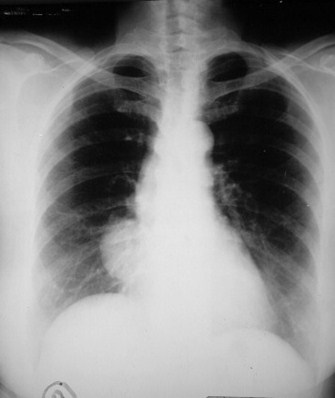
Where is this patient’s heart?
This patient hashad the left lungremoved – apneumonectomy.Fibrous tissue nowfills the lefthemithorax. Theheart is “invisible”because it nolonger borders onan air-filled lung. Itnow borders onsoft tissue densitywhich is the samedensity as theheart. Therefore,the edge of theheartdisappears=thesilhouette sign.
Using the Silhouette Sign
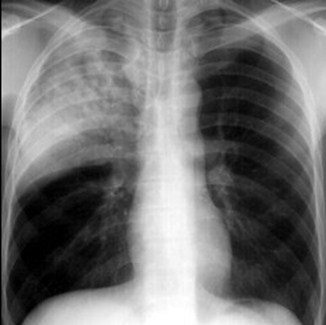
The mass (red arrow)silhouettes the rightheart border which isto say there is nolonger an edge of theright heart seen. Thatmeans the mass is (a)touching the rightheart border (the massis anterior) and (b) themass is the samedensity as the heart(fluid or soft tissuedensity). The mass isa thymoma.
Where in the chest is this mass?
Using the Silhouette Sign
Hot links on this page
Air Bronchogram
Bronchi are not visible since their walls arethin, they contain air, are surrounded by air
When something of fluid density fillsalveoli, air in bronchus becomes visible,e.g.
Pulmonary edema fluid
Blood
Gastric aspirate
Inflammatory exudate
Air Bronchogram
The visibility of air in the bronchi becauseof surrounding airspace disease is calledan “air bronchogram”
An air bronchogram is almost always asign of airspace disease
The black branchingstructures are theresult of air in thebronchi, now visiblebecause densityother than airsurrounds them (inthis case it isinflammatory exudatefrom a pneumonia).
Solid Spheres vs. Hollow Tubes
A. Solid spheres are homogeneous from oneside to other
Blood vessels and masses
B. Hollow tubes have a lower density incenter
Bronchi and cavities
A
B
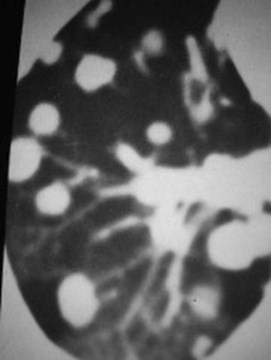
Solid spheres or hollow tubes?
There are multiplenodules visible onthe CT scan of thechest in this patient.
In most cases thenodules are due tometastases from aprimary malignancyin an organ otherthan the lung.
Hot links on this page
Diseases with Multiple Lung Nodules
Hot links on this page
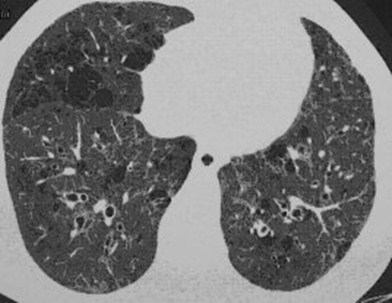
Solid spheres or hollow tubes?
There aremultiple tube-likestructures seenin the lung of thisperson.
These are dilatedbronchi inbronchiectasis.This raises anentirely differentset ofpossibilities thanthe multiplenodules seen inthe last case.
Hot links on this page
Disease with Multiple CysticStructures
Hot links on this page
Parenchymal Lung Disease
Two Major Types
Alveolar (airspace)
Interstitial
Alveolar Lung Disease
Has air bronchograms
Fluffy and indistinct
Confluent and homogeneous
May have segmental or lobar distribution
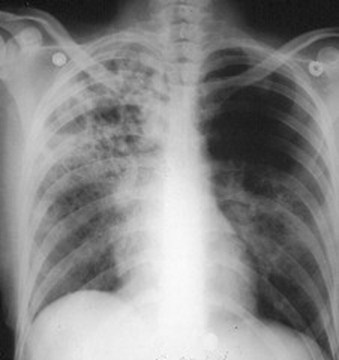
Pulmonary edema
This disease isfluffy and indistinctin its margins, it isconfluent andtends to behomogeneous. Inboth upper lobes,you can see airbronchograms.This is an alveolar(airspace) disease,in this casepulmonary edemaon a non-cardiogenic basis.
Hot links on this page
Common Alveolar Lung Diseases
Hot links on this page

Interstitial Lung Disease
Discrete
Inhomogeneous
No air bronchograms
Made up of lines (reticular) or dots(nodular) or both (reticulonodular)


Interstitial disease – discrete,inhomogeneous, no airbronchograms
Airspace disease – fluffy,indistinct, homogeneous,contains air bronchograms
Interstitial versus Airspace Disease
Common Interstitial Lung Diseases
Hot links on this page

Opacified HemithoraxThree Causes
Atelectasis
Opacified hemithorax from volume loss
Shift of heart and mediastinal structurestoward opacified hemithorax

Atelectasis of right lung – shift of the mediastinal structuresTOWARD the side of opacification
Pleural Effusion
Opacified hemithorax from largeeffusion
Shift of heart and mediastinalstructures away from side of opacifiedhemithorax

Large right pleural effusion - shift of the mediastinal structuresAWAY from the side of opacification
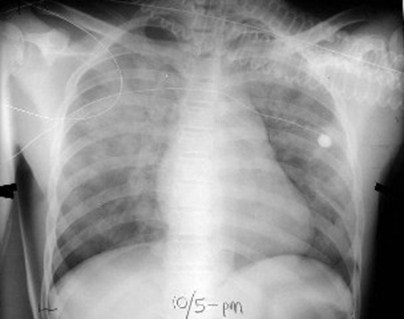
Pneumonia
Opacified hemithorax
No shift
Air bronchograms
Pneumonia of LUL – no shift of the mediastinalstructures to either side; multiple air bronchograms
Congestive Heart FailureFour Reliable Signs
Kerley B lines
Pleural effusions
Fluid in the fissures
Peribronchial cuffing
Not cardiomegaly
Not cephalization
Kerley B Lines
Four Reliable Signs of CHF
Short (1 -2 cm)white lines atthe lungbases,perpendicularto the pleuralsurfacerepresentingdistendedinterlobularsepta

Pleural Effusions
Four Reliable Signs of CHF
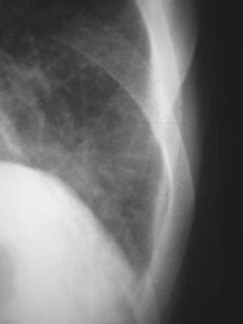
Fluid in the fissures
Four Reliable Signs of CHF
Fluid in theminor fissure.The fissuresmay be seennormally butthey shouldbe about asthin as a linedrawn with asharpenedpencil.
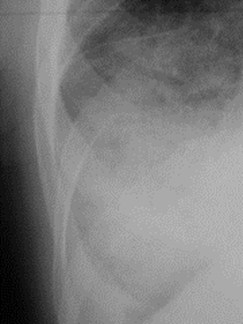
Peribronchial cuffing
Four Reliable Signs of CHF
Fluid in thewalls of thebronchi makethem visibleand producenumerous“doughnut”densitiesthroughoutthe peripheryof the lung.
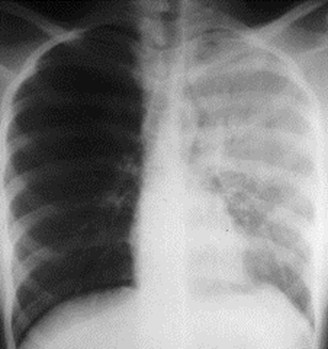
Pneumothorax
Must see visceral pleural white line
Absence of lung markings peripherally
Shift of mediastinal structures
None=simple pneumothorax
Away from pneumothorax=tensionpneumothorax
Never a shift toward side of pneumothorax

Visceral pleural white line marks the edge of the lung
Cavitary Lung LesionsDifferentiation
Thickness of the wall
Inner margin of the cavity
Air-fluid level
Carcinoma
TB
Abscess
Thickness of
Wall
Inner Margin
A|F Level
Thick
Thick
Thin
Nodular
Smooth
Smooth
No
Yes
+/-
Cavities
Cavities

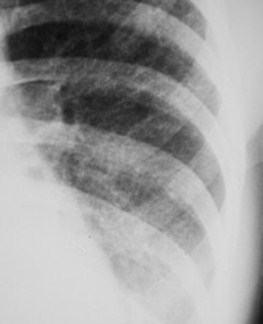
Thick-walled with nodular inner margin –carcinoma of the left lower lobe

Thick-walled with smooth inner margin –RUL abscess
Thin-walled with smooth inner margins, RUL –Tuberculosis
Carcinoma
TB
Abscess
Thickness of
Wall
Inner Margin
A|F Level
Thick
Thick
Thin
Nodular
Smooth
Smooth
No
Yes
+/-
Cavities
Cavities
