Plain FilmsOf the AbdomenAn Approach
Plain FilmsOf the AbdomenAn Approach
© William Herring, MD, FACR
Lecture Map
Normal Gas Pattern
Obstruction Series
Abnormal Gas Pattern
Aunt Minnies
Extraluminal Air
What to look for
Soft Tissue Masses
Calcifications
What to Examine
Gas pattern
Extraluminal air
Soft tissue masses
Calcifications

Normal Gas Pattern
Stomach
Always
Small Bowel
Two or three loops of non-distended bowel
Normal diameter = 2.5 cm = 1 US quarter
Large Bowel
In rectum or sigmoid – almost always


Gas instomach
Gas in a fewloops ofsmall bowel
Gas inrectum orsigmoid
Normal Gas Pattern
Normal Fluid Levels
Stomach
Always (except supine film)
Small Bowel
Two or three levels possible
Large Bowel
None normally

Erect Abdomen
Alwaysair/fluid levelin stomach
A fewair/fluidlevels insmall bowel
Large vs. Small Bowel
Large Bowel
Peripheral
Haustral markings don't extendfrom wall to wall
Small Bowel
Central
Valvulae extend across lumen
Maximum diameter of 2"

Complete AbdomenObstruction Series
Supine
Prone or lateral rectum
Erect or left decubitus
Chest - erect or supine
Complete AbdomenSupine
Looking for
Scout film for gaspattern
Calcifications
Soft tissue masses
Substitute – none

Complete AbdomenProne
Looking for
Gas in rectum/sigmoid
Gas in ascending anddescending colon
Substitute – lateralrectum

Complete AbdomenErect
Looking for
Free air
Air-fluid levels
Substitute – leftlateral decubitus

Left Lateral Decubitus View

Amateur Style
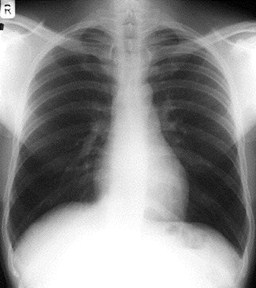
Complete AbdomenErect Chest
Looking for
Free air
Pneumonia at bases
Pleural effusions
Substitute – supinechest
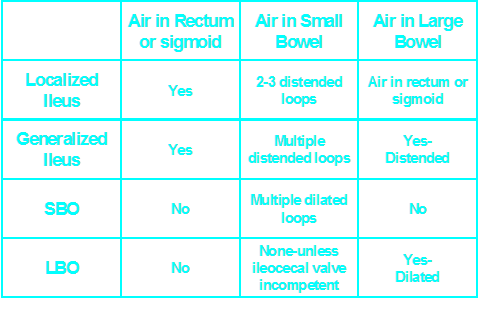
Abnormal Gas Patterns
Functional Ileus
Localized (Sentinel Loops)
Generalized adynamic ileus
Mechanical Obstruction
SBO
LBO
Laws of the Gut
Loops proximal to an obstruction willbe dilated
Loops distal to an obstruction will bedecompressed or airless
Most dilated loop will either be:
Most distended to start
Bowel just proximal to the obstruction
One or two persistently dilated loops oflarge or small bowel
Gas in rectum or sigmoid
Localized IleusKey Features
Sentinel Loops

Supine

Prone
PancreatitisUlcer
Diverticulitis
Cholecystitis
Appendicitis
UlcerUreteral calculus
Sentinel Loops
Localized IleusPitfalls
May resemble earlymechanical SBO
Clinical course
Get follow-up


Gas in dilated small bowel and largebowel to rectum
Long air-fluid levels
Only post-op patients havegeneralized ileus!
Generalized IleusKey Features


Generalized Adynamic Ileus
Supine
Erect
Is It An Ileus?
Is the patient immediately post-op?
Are the bowel sounds absent orhypoactive?
If “no,” then it isn’t an ileus
Patients don’t present to the ER with ageneralized adynamic ileus!
Mechanical SBOKey Features
Dilated small bowel
Fighting loops
Little gas in colon, especially rectum
Key: disproportionate dilatation of SB

SBO
Mechanical SBOCauses
Adhesions
Hernia*
Volvulus
Gallstone ileus*
Intussusception
*Cause may be visible on plain film
Mechanical SBOPitfalls
Early SBO mayresemblelocalized ileus -get F/O
Mechanical LBOKey Features
Dilated colon to point of obstruction
Little or no air in rectum/sigmoid
Little or no gas in small bowel, if…
Ileocecal valve remains competent
LBO

Supine

Prone
Mechanical LBOCauses
Tumor
Volvulus
Hernia
Diverticulitis
Intussusception
Mechanical LBOPitfalls
Incompetent ileocecal valve
Large bowel decompresses into smallbowel
May look like SBO
Get BE or follow-up
Carcinoma of Sigmoid – LBO –Decompressed into SB

Prone

Supine
Aunt Minnies


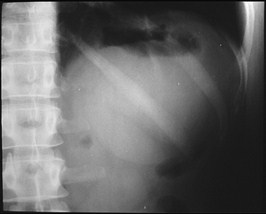
Air inbiliarytree
SBO
Gallstone
Gallstone Ileus

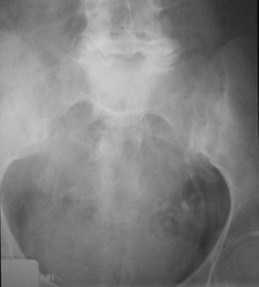
Post-op C-sectionAdynamic Ileus
Soft tissuemass inpelvis
Midlinesutures
Dilatedsmall andlarge boweldisplacedfrom pelvis

Sigmoid Volvulus

Mesenteric Occlusion
Abnormal Gas PatternsIleus and Obstruction
Localized ileus
Generalized ileus
Mechanical SBO
Mechanical LBO
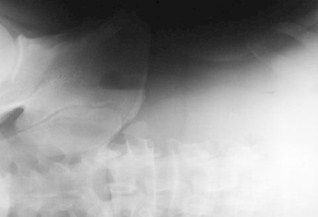
Extraluminal AirFree Intraperitoneal Air
Signs of Free Air
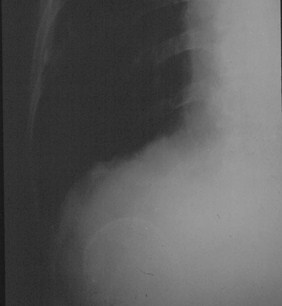
Air beneath diaphragm
Both sides of bowel wall
Falciform ligament sign

ERECT
Crescentsign
Free Intraperitoneal Air


Free Intraperitoneal Air
Air on both sides ofbowel wall – Rigler’sSign

Free Intraperitoneal Air
FalciformLigamentSign

Football sign
Free AirCauses
Rupture of a hollow viscus
Perforated ulcer
Perforated diverticulitis
Perforated carcinoma
Trauma or instrumentation
Post-op 5–7 days
NOT perforated appendix

Air in Lesser Sac
Extraperitoneal Air

Intermission
There is no such thing as a “non-specific”gas pattern
It is either normal or abnormal
Adynamic Ileus is overcalled
Only occurs in post-op patients
Take notes in conference
Soft Tissue Masses
Soft Tissue Masses
Hepatosplenomegaly
Plain films poor for judging liver size
Tumor or cyst
Bowel displacement
Paucity of gas
Pad sign
•Extrinsic compression of bowel

Splenomegaly

Myomatous Uterus

Bladder Outlet Obstruction – pre- and post- cath

Hourslater

Hourslater
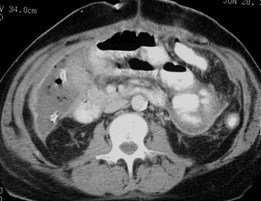
Mass in Cologastric Space - Pancreatic Pseudocyst


Right Renal Cyst


RLQ Abscess


Free Peritoneal Fluid- Bladder Ears

AbdominalCalcifications
AbdominalCalcifications
Abdominal CalcificationsPatterns
Rimlike
Linear or track-like
Lamellar
Cloudlike
Rimlike Calcification
Wall of a hollow viscus
Cysts
Renal cyst
Aneurysms
Aortic aneurysm
Saccular organs e.g. GB
Porcelain Gallbladder


Renal Cyst
Gallbladder Wall
Linear or Track-like
Walls of a tube
Ureters
Arterial walls

Atherosclerosis
Calcification Vas Deferens
Lamellar or Laminar
Formed in lumen of a hollow viscus
Renal stones
Gallstones
Bladder stones

Stone in Ureterocoele
Staghorn Calculi

Cloudlike, Amorphous, Popcorn
Formed in a solid organ or tumor
Leiomyomas of uterus
Ovarian cystadenomas

Nephrocalcinosis
Myomatous Uterus

Unknowns

Dermoid
Jackstone Calculus


Calcific Pancreatitis

Prostatic Calcification

Renal cyst
Porcelain Gallbladder

What to Examine
Gas pattern
Extraluminal air
Soft tissue masses
Calcifications