
Urinary Tract Infections:Imaging
Mindy M. Horrow, MD, FACR, FSRU, FAIUM
Director of Body Imaging Einstein Medical Center
Professor of Radiology Jefferson Medical College
January, 2013
Outline
Pathophysiology
Imaging Approach
Pyelonephritis
–Acute
–Chronic
Abscess
–Acute versus Chronic
– Renal
–Peri-renal
Pyonephrosis
Emphysematous Infections
Chronic infectious/inflammatory processes
Specific Infections
–Tuberculosis
–Fungus
–Opportunistic Infections
Pathophysiology
Bacterial infection, usually ascending. In childrentypically due to reflux. In adults occurs without reflux.(Some forms of E. coli elaborate a protein whichfacilitates adhesion to urothelial cells.)
Women > men if < 50 years. After this age menpredominate due to urinary stasis from BPH.
Hematogenous spread of infection much less common.
Predisposing conditions: reflux, obstruction, calculi,altered bladder function, altered host resistance,pregnancy, congenital anomalies of urinary tract
Pathophysiology
Symptoms include: fever, flank pain, chills, nausea,vomiting, malaise
Pathogens are usually gram negative enterics: E. coli,Proteus mirabilis, Pseudomonas aeruginosa, Klebsiella
Pathology: acute bacterial infection manifested byinfiltration of renal interstitium with neutrophils, causingswelling, hyperemia and microabscesses
Imaging Approach
Diagnostic imaging unnecessary if diagnosis is clinicallycertain and patient responds promptly to antibiotics
Rationale for imaging is to look for underlyingabnormality which predisposes patient to infection, or todiagnose a complication
CT with contrast is usual study of choice forcomplications, but US can be useful for obstruction andabscess
Other: Tc- 99m DMSA, MRI, retrograde pyelography,antegrade pyelography, VCUG (especially in children)
Normal Nephrographic Progressionon Contrast CT
Vascular
–10 – 15 seconds after beginning IV administration
Cortical (cortico-medullary)
–20 – 45 seconds
Nephrographic
–45 – 100 seconds
Excretory
–2 – 3 minutes
Timing depends upon amount and rate of contrastadministration, cardiac output, integrity of renalvasculature and renal function
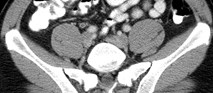


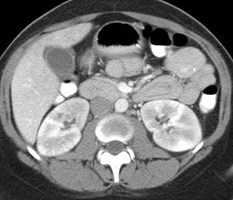
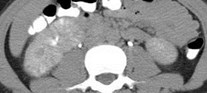
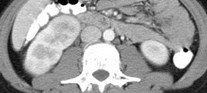
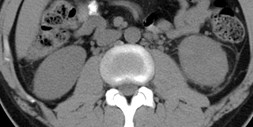
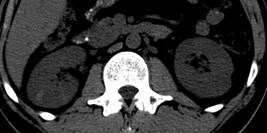
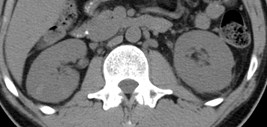
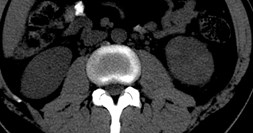
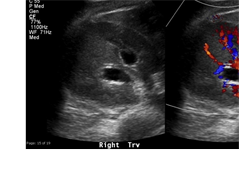
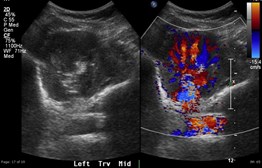
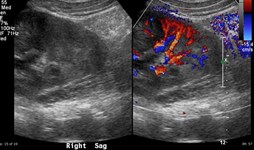
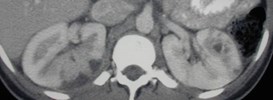
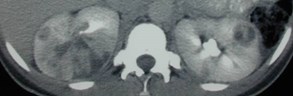
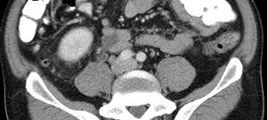
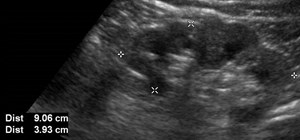
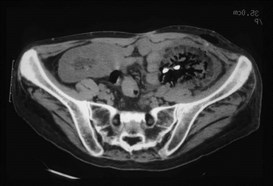
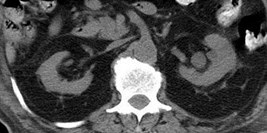
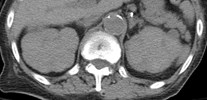
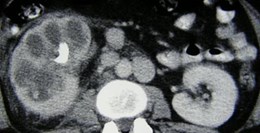
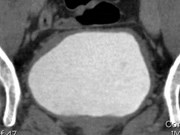
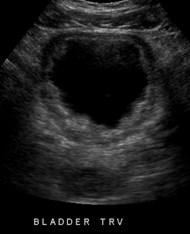
42 year old male with right sided pain, wbc 15.4,
> 100,000 gram negative rods in urine
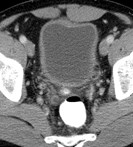
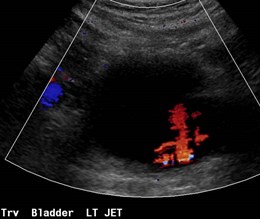
Ureterocystitis(pyelitis)
Infected organisms in bladder migrate up ureter tocollecting system.
Endotoxins produced by bacteria thought to inhibitureteral peristalsis, creating a functional obstruction
This obstruction impedes forward flow of urine whichnormally protects against spread of infection to uppertracts
Visualized as thickening and enhancement of urotheliumof bladder, ureter and renal pelvis and may be seenoccasionally before renal parenchymal changes occur.

Acute Pyelonephritis
Most common renal infection
Usually responds quickly to antibiotics and thus imagingis negative in almost 75%
Involved kidney is enlarged with patchy distribution,often wedge shaped distribution
Use descriptive modifiers: focal or global, unilateral orbilateral, diffuse or focal enlargement
Ascending disease spreads from pelvis to medullawhere relatively low oxygen tension allows spread
Hematogenous disease results in focal corticaldistribution
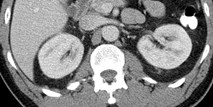
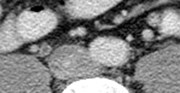
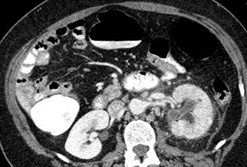
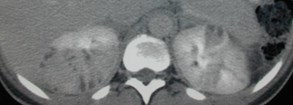
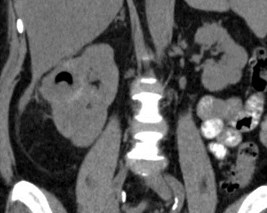
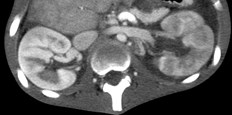
Acute Pyelonephritis: Contrast CT
Hallmark is striated nephrogram with parenchymal wedgeshaped areas of hypoperfusion and poor cortico-medullarydifferentiation due to localized enhancement and excretion ininflamed areas
Excretory phase: smaller wedge shaped hypodensities oftenfocal hyperdensities parallel to tubules. Probably representlocalized “delayed pyelograms” secondary to tubularobstruction by inflammatory cells and debris. Thus, if earlyphase is confusing or even normal, get delayed excretoryimages.
Other: Soft tissue stranding, thickening of Gerota’s fascia,thickening and hyper-enhancement of urothelium, mildcaliectasis and ureteral dilatation, obliteration of renal sinus,calyceal effacement
Non-contrast CT: enlargement, perinephric stranding, fascial thickening, milddilatation (as in acute stone disease)



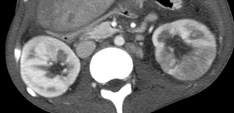
Bilateral Pyelonephritis (transient small bowel intussusception)
Striated Nephrogram
Bands of alternating increased and decreased attenuationparallel to axis of tubules
Unilateral causes:
–Ureteral obstruction
–Acute pyelonephritis: cellular inflammation causes regions ofincreased parenchymal pressure which demonstrates decreasedenhancement. On delayed imaging, same areas may haveincreased attenuation secondary to tubular stasis
Bilateral causes:
–Acute pyelonephritis
–Tubular obstruction
–Hypotension
–Autosomal recessive polycystic kidney disease
–Rhabdomyolysis
Saunders. Radiographics. 1995;15:1069

Early imaging at routine and narrow windows andexcretory imaging
Acute Pyelonephritis
Striated nephrograms with “flip flop”
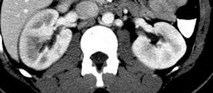
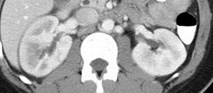
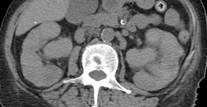
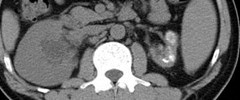
Left flank pain: Stone Search CT
Findings: thickening of Gerota’s fascia and perinephric strandingL > R, non contrast “striated nephrogram”
Pyelonephritis




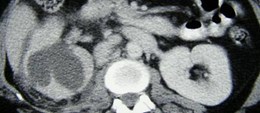
Right Flank Pain
Cortical Rim Sign
Renal Infarcts
Delayed

Acute Pyelonephritis
Enlarged kidney
Diffusely delayed nephrogram
Hydronephrosis
Enhanced urothelium
Perinephric fluid
Thickening of Gerota’s fascia
Lymphadenopathy
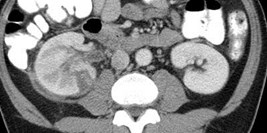
Pregnant patient with right flank pain and fever
Acute Pyelonephritis
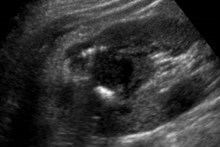
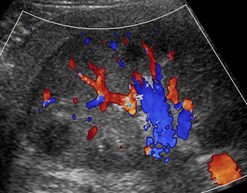
Acute Pyelonephritis: US
Majority of kidneys are normal.
Most common finding is enlargement
More focal findings are often subtle. Typically abnormalregions are hyperechoic (? Hemorrhagic) , but may also behypoechoic or mixed. Color or power Doppler will showdecreased flow.
Loss of cortico-medullary distinction
Poorly marginated masses
Mild caliectasis, urothelial thickening
Ultrasound contrast agents may be useful in this diagnosis,but not available in the United States
US with power Doppler less sensitive than Tc-DMSA, MR orCT
Farmer. Clin Radiol 2002;57:483
Dacher AJR 1996;166:1451
Majd Radiology 2001`;218:101

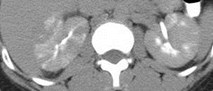
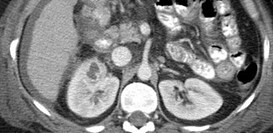
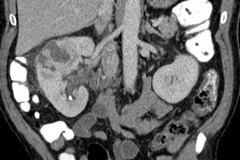
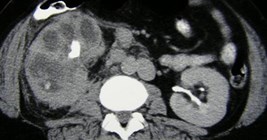
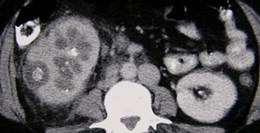
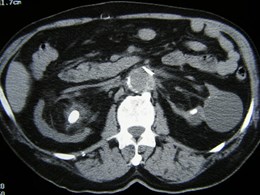
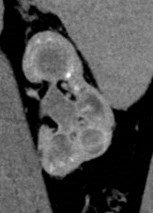
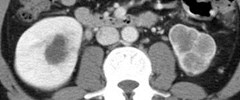
Numerous regions of pyelonephritis and multiplecoalescing necrotic areas without delayed enhancement orexcretion: Abscess Formation in Progress
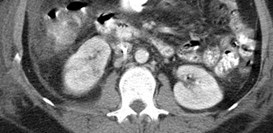
Acute Pyelonephritis 2 weeks later
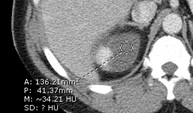
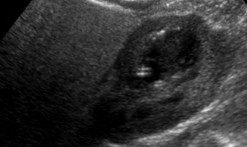
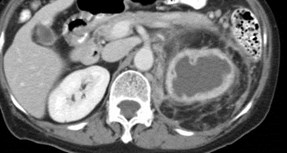
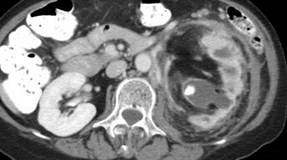
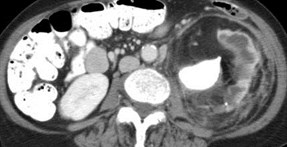
Renal Abscess

Renal Abscesses withperinephric extension: fluid,urothelial enhancement,calculus, mild caliectasis,thickening of Gerota’s fascia

R L
Sag R upper Trv R upper


Gas containingrenal abscess
High density foci indicate a hemorrhagic component to the inflammation.
Abscess in region of pyelonephritis
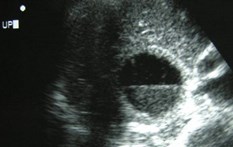
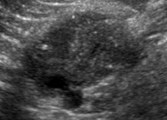
Renal Abscess
CT is most accurate modality for diagnosis and follow-up
Severe vasospasm and inflammation result inliquefaction and necrosis evolving into an abscess
US: relatively sonolucent with poor through transmissionand appearance of a complex mass
CT: low attenuation rounded “mass” with irregular oftenenhancing wall or pseudocapsule, occasional gas,adjacent perinephric inflammation
Diabetics acount for ¾ of all renal abscesses
Up to 20% of patients with an abscess may havenegative urine cultures, presumably reflecting theconfined nature of the abscess.
Thornbury. Urol Radiol 1991;12:209


Acute Pyelonephritis
3 ½ years later
Chronic Scarring




(1) marked cortical scarringopposite medullary pyramids
(2) blunted calyces, right upperpole papillary necrosis



ChronicPyelonephritis
Chronic Pyelonephritis
Usually due to reflux of infected urine in childhood.
Classic findings
–focal scars in polar regions of kidney with associated calycealdistortion
–Global atrophy with diffuse dilatation of collecting system, often withsignificant fatty replacement of renal sinus
Adults followed long term with severe infections maydemonstrate focal or generalized scarring with calycealclubbing as in papillary necrosis
Imaging may show focal regions of compensatory hypertrophywhich appear mass-like
“Reflux Nephropathy”
Cortical defects can occur after pyelonephritis
Most common in young children, especially those lessthan 2 years
More and larger defects in those with reflux
Describes both the acute damage to the kidney by refluxof infected urine and the long term sequelae
Can lead to hypertension and renal failure


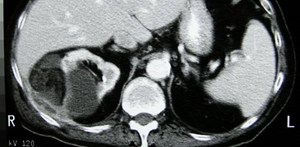
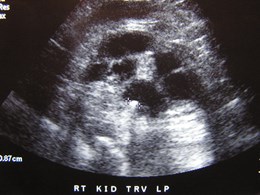
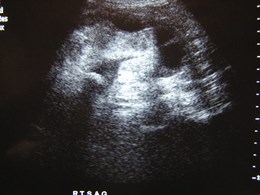
Abscess in calyceal diverticulum
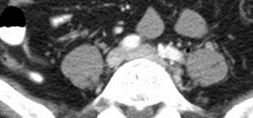



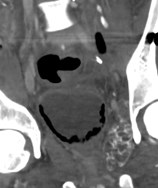
Emphysematous Pyelitisand Ureteritis with multiplecalculi
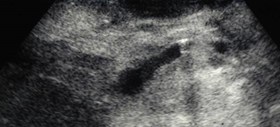


R Sag R Trv
Sag R Ureter
Emphysematous Pyelitis and Ureteritison ultrasound, confirmed on CT

Emphysematous: pyelitis, ureteritis, cystitis
Emphysematous Pyelonephritis
Second renal transplant in a diabetic
Emphysematous Urinary TractInfections
Emphysematous pyelonephritis:
–fulminant gas forming infection of parenchyma, a necrotizingpyelonephritis with 70% mortality
–Probably due to a urinary tract infection occurring in a glucose richsubstrate in a patient with vascular impairment and/or immunecompromise
–Rapid destruction or renal parenchyma, residual fibrous septioutlined by gas
Emphysematous pyelitis: gas in collecting system, betterprognosis, associated with diabetes, obstruction
–Bubbles and loculated collections of gas, gas withing wall
–Tissue injury occurs in patients with more intact immune system,exudate accumulates and limits spread of infection resulting in anabscess which protects against further spread
Organisms: E. coli, Klebsiella, Aerobacter, Proteus
Roy. Radiology 2001;218:647
Wan. Radiology 1996;198:433



Gas Containing Renal Calculi
Rare phenomenon
Should consider as an emphysematousinfection
Associated with diabetes mellitus
Patients present with UTI, E coli in urine
Manny. Urology 2012;80:1203

Initial study 2 weeks later with fever

Sagittal and transverse views of left kidney
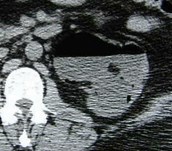
Pyonephrosis


Distant history cervical carcinoma, nausea, vomitingand right upper quadrant pain, for gallbladder US
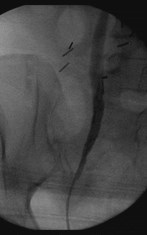
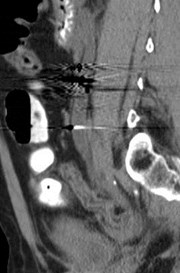

Smooth, benign right ureteral stricture from priorXRT, pyonephrosis at percutaneous nephrostomy
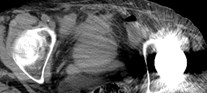




Bilateral Pyonephrosis



Pyonephrosis, Emphysematous Pyelitis and Cystitis
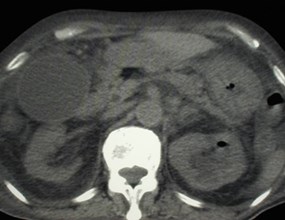
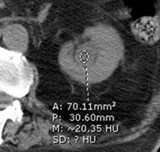
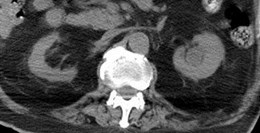
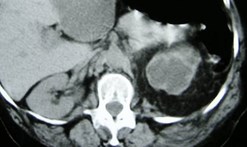
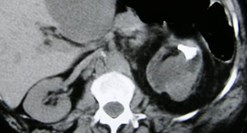
XanthogranulomatousPyelonephritis
1.Right Renal Enlargement
2.Central calculus within acontracted pelvis
3.Non-functioning
4.Perinephric inflammation
5.Dilated calyces


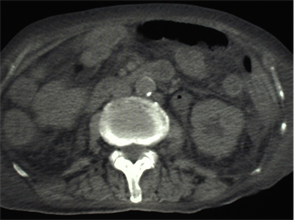
Xanthogranulomatous Pyelonephritis


Several years after nephrectomy, bulging flank
Recurrent inflammatory mass from XGPN


Focal Xanthogranulomatous Pyelonephritis
Xanthogranulomatous Pyelonephritis
Uncommon chronic renal parenchymal infection
Pathology
–Soft yellow nodules composed of foamy lipid laden macrophages.Usually diffuse but may be focal. Peri-renal extension with abscessand fistula formation are common
–Contracted renal pelvis, thin cortex, unilateral enlargement,nephrolithiasis (frequently staghorn), calyces if preserved are dilated
–Focal form confined to one pole or calyx
Proposed etiologies: chronic obstruction calculus, ineffectivelytreated chronic urosepsis, altered lipid metabolism, arterialinsufficiency, venous occlusion
Rare manifestations: renal atrophy, absent calculi
Xanthogranulomatous Pyelonephritis
Clinical
–5th to 7th decades, women > men
–Vague constitutional sx, 80% pyuria and proteinuria, flankpain and possible mass
–Treatment: Total Nephrectomy
Organisms
–E.coli, proteus mirabilis, klebsiella, pseudomonas
–Sterile urine in one third
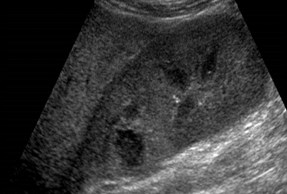
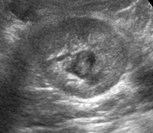
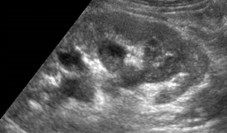
Xanthogranulomatous Pyelonephritis
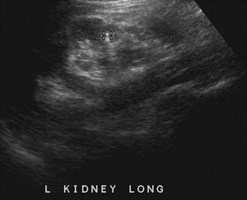
Ultrasound:
–Large kidney with multiple anechoic or hypoechoic fluid collectionswhich are the dilated calyces and/or parenchymal destruction
–Pelvic contraction with increased echogenicity from calculi
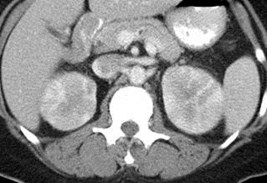
CT:
–Large kidney, parenchyma replaced by multiple low attenuationrounded masses.
–Central calculus and calyceal calculi, contracted pelvis
–Thickening Gerota’s fascia, extension into peri-renal, pararenal,psoas, skin
–Only enhancement in periphery secondary to inflammatoryvascularity but poor or no renal function.
Hayes. Radiographics 1991;11:485

Replacement Lipomatosis
Replacement Lipomatosis(Replacement fibrolipomatosis)
Extreme form of renal sinus lipomatosis in which infection withchronic hydronephrosis and calculi are associated with severeparenchymal atrophy
Pathology: Large kidney, gross fibrofatty appearance with thincortex, hydro or pyonephrosis and pyelonephritis. Reniformshape maintained, marked proliferation of hyperplastic fat in renalsinus
US: expanded echogenic mass like sinus calculi, may bedifficult to appreciate thin hypoechoic cortex
CT: most accurate, calculi, altrophic parenchyma, expandedcentral sinus fat may extend into perinephric space
Major differential diagnosis is XGPN which expands kidney withfluid or soft tissue density, two entities may co-exist
Karasick Radiology 2000;215:754


Replacement Lipomatosis and XGPN ?



History of HIV
TRV TRV
AIDS and the Urinary Tract
Recurrent urinary tract infections in 50%
Multiple punctate calcifications due todisseminated pneumocystis carinii may occur inkidneys, lymph nodes, spleen , liver and adrenalglands
Similar calcifications occur with CMV and MAIinfections

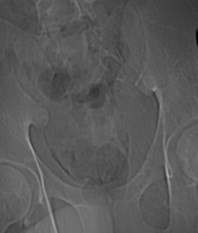
Tuberculosis of the Urinary Tract
1.Hydronephrosis
2.Upper pole cavity
3.Ureteral fibrosis with strictures
4.Irregular bladder wallthickening
5.Non functioning left kidney


Autonephrectomy “Putty” Kidney




Putty Kidney = Autonephrectomy


“Putty Kidney” secondary toTuberculosis



Focal parenchymal calcifications associated with cortical scars
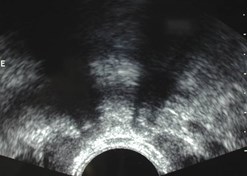
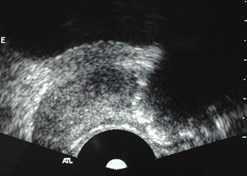

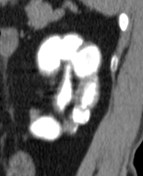
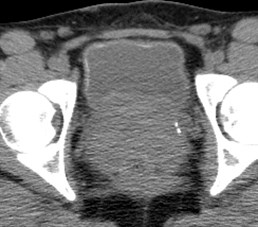
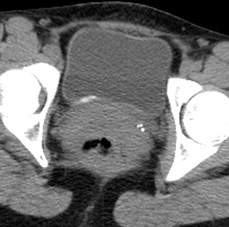
Vas deferens and prostate calcifications

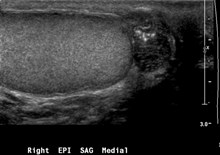
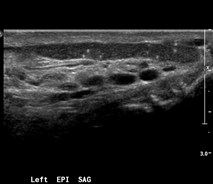
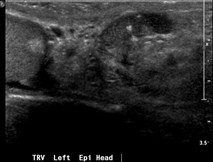
TB granulomas: epididymi, seminal vesicles

Tuberculosis and the Urinary Tract
Renal TB 2° hematogenous infection from lungs. GU systemis second most common site of infection occurring in 4 – 8%with pulmonary TB but only 5% have active pulmonary TB
–Compromised host immunity years later causes reactivation
Parenchymal granulomas coalesce and rupture into calyx andremainder of collection system. Causes papillary necrosis.Fibrosis in healing phase causes strictures
–Focal hydrocalyx calculi 2° infundibular stricture
–Advanced disease: cavities that communicate with collecting system,cortical scarring, dystrophic amorphous calcifications
–Autonephrectomy: hydronephrotic kidney, calcified cast appearance
•Small calcified, non-functioning kidney
•Large if hydronephrosis occurs secondary to fibrosis at UPJ
Gibson. Radiographics 2004;24:251
Kawashima Radiographics 1997;17:851
Tuberculosis and the Urinary Tract
Ureter: commonly involved. May appear ragged, dilatedwith filling defects and ulcerations. With advanceddisease chronic fibrosis and foreshortening (pipe-stem ureter). Differential dx includes calculous diseaseand schistosomiasis.
Bladder- reduced capacity, wall thickening, reflux
Genitalia:
–Men: calcifications in prostate seminal vesicles and vasdeferens, TB epididymo-orchitis
–Women: endometrial adhesions with deformity andobliteration of endometrial cavity, obstruction andcalcifications of fallopian tubes
Harisinghani. Radiographics 2000;20:449
Schistosomiasis
4-09 6-09
Schistosomiasis
Second most common parasitic infection after malaria
Parasitic infection by trematodes of genus Schistosoma
–First host is water snail
–Humans and other mammals infected through direct contact withinfested water
Penetrates skin and passes via lymphatics and thoracicduct to right heart to lungs, left heart, liver (where theymature and copulate spreading via venous plexus tobladder and prostate where they produce eggs
–Eggs are highly antigenic, producing intense granulomatous reaction
Shebel. Radiographics 2012;32:1031-46
Imaging of Schistosomiasis
Predominately involves ureters and bladder
Ureteral strictures occur in intravesical segment ofureter, progressing proximally
Mural calcification bladder wall and fine ureteralcalcification
–Degree of calcification correlates with volume of ova
Lead to decreased peristalsis, hydronephrosis,hydroureter
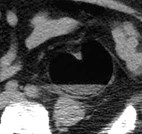
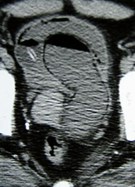
Hemorrhagic Cystitis

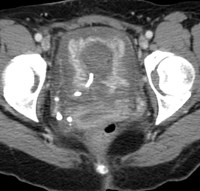
Fever and gross hematuria

2 months later
Differential Diagnosis Bladder WallThickening
Diffuse:
–muscular hypertrophy, cystitis (acute and chronic),neoplasm, amyloidosis
Focal:
–Neoplasm: urothelial, squamous, adenocarcinoma,lymphoma, metastases
–Infectious/inflammatory: TB, schistosomiasis, cystitis,malcoplakia, cystitis cystica/glandularis, fistula
–Medical: endometriosis, amyloidosis, trauma (hematoma)
Francica etal. JUM 2008;27:887-894
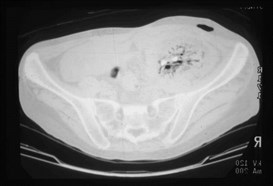
Pyelonephritis and EmphysematousCystitis
General References
Craig WD, etal. Pyelonephritis: Radiologic-Pathologic Review.Radiographics. 2008;28:255-276
Foxman B. Epidemiology of urinary tract infections: incidence, morbidity,and economic costs. Am J Med 2002;113(suppl 1A):5S-13S.
Vourganti S., etal. Ultrasonographic evaluation of renal infections. RadiolClin North Am 2006;44:7630775.
Loffroy R, etal. Xanthogranulomatous pyelonephritis in adults. Clin Radiol2007;62:884-890
Wang LJ, etal. CT features of genitourinary tuberculosis. J. ComputAssist Tomogr 1997;21:254-258
Shebel HM, etal. Genitourinary Schistosomiasis: Life Cycle andRadiologic-Pathologic Findings. Radiographics 2012; 32:1031-1046