
The Peritoneum
Mindy M. Horrow, MD, FACR, FSRU
Director of Body Imaging, EMC
Professor of Radiology Jefferson Medical School
March 14, 2013
Outline
•Definitions
•Anatomy
•Pathology
Definitions
•Ligament: 2 folds of peritoneum supporting astructure in peritoneal cavity, usually named for 2structures it connects, for example: gastrohepaticligament
•Omentum: 4 layers of peritoneum
–Greater: drapes from greater curvature of stomach,merging into transverse mesocolon
–Lesser: connects lesser curvature of stomach with liver
•Mesentery: 2 peritoneal folds connecting a portionof bowel to the retroperitoneum
–Transverse mesocolon, small bowel mesentery,sigmoid mesocolon
Peritoneum
•Lines a body cavity that extends fromabdomen to pelvis
•Parietal peritoneum covers abdominal wall
•Visceral peritoneum covers bowelsurfaces forming the tunica serosa.
•In non-pathologic states peritoneal cavitycontains only small amount of fluid.
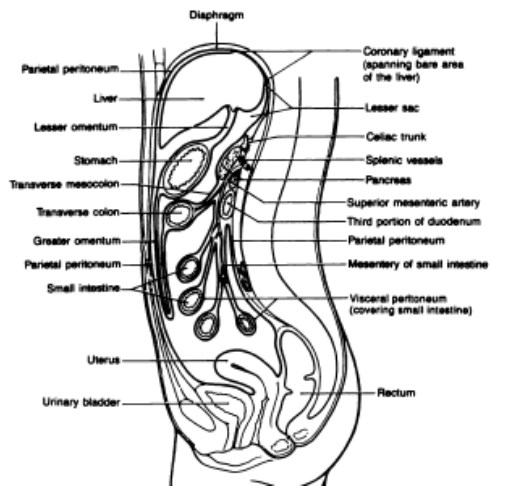
Radiographics 1992;12:1051
Omentum
•Greater Omentum: drapes inferiorly from greatercurvature of stomach and proximal duodenum,anterior to small bowel to merge with transversemesocolon. Contains variable amounts of fat.Serves to limit spread of infectious processes.
•Lesser Omentum: connects lesser curvature ofstomach and proximal duodenum with liver.Contains blood vessels, nerves and lymphnodes
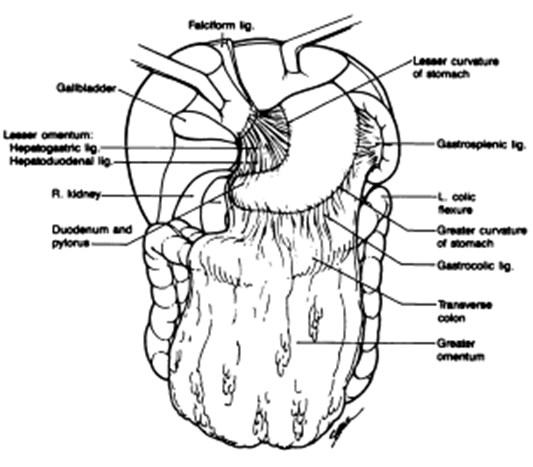
Radiographics 1992;12:1051
Small Bowel Mesentery
•Fan shaped double peritoneal fold
•Suspends jejunal and ileal small bowelloops from posterior abdominal wall,running from left upper quadrant to rightlower quadrant
•Contains vascular and lymphaticstructures
•Encases bowel loops, forming the visceralperitoneal coat
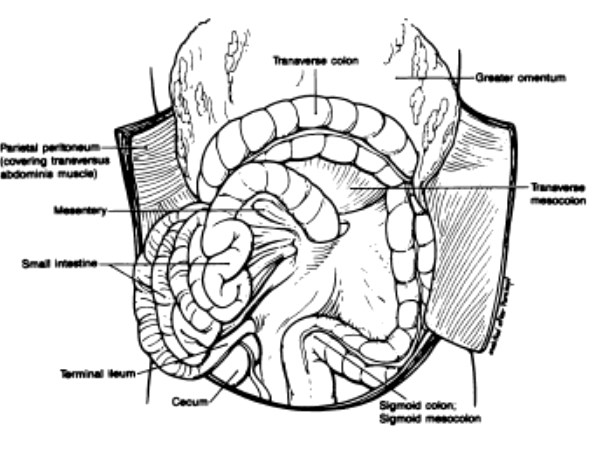
Radiographics 1992;12:1051
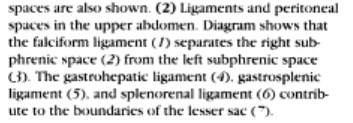
Supramesocolic Ligaments andSpaces
•Left subphrenic space: between diaphragm andstomach, common location for fluid, abscesses,blood, gastric processes. Connects toperisplenic space, gastrohepatic recess,separated from right subphrenic spaces byfalciform ligament which attaches ventral liver toanterior abdominal wall and containsligamentum venosum (obliterated umbilical vein)
Supramesocolic Ligaments andSpaces
•Right Perihepatic Space: right triangular ligamentdivides posterior aspect of right perihepatic spaceinto right subphrenic and subhepatic spaces
–Subphrenic space: between liver and diaphragm,anterior aspects communicates with lesser sac viaforamen of Winslow
–Posterior subhepatic space: also known as Morisonpouch is most dependent portion of abdomen in asupine patient
–Bare area of liver is devoid of peritoneum, lies betweenreflections of right and left coronary ligaments and iscontinuous with anterior pararenal space to theretroperitoneum
Lesser Sac
•Communicates with remainder ofperitoneum via epiploic foramen ofWinslow
•Contains 3 recesses: superior, splenic,inferior
•Isolated fluid in lesser sac usually relatedto pancreatitis or perforated gastric orduodenal ulcer
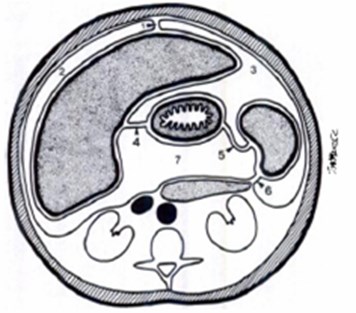
Radiographics 1995;15:755
Inframesocolic Mesenteries andSpaces
•Transverse mesocolon: common pathway ofspread from pancreas to inferior border oftransverse colon
•Greater Omentum: involvement by inflammatoryprocesses, primary or metastatic neoplasticprocesses, hematomas, cysts
•Small Bowel Mesentery: from ligament of Treitzto ileocecal valve
•Sigmoid Mesocolon and inter-sigmoid recessalong its undersurface
Radiographics1995;15:755



Injection of peritoneal dialysis catheter with contrast
Bare Area
R and L Subphrenic
Perisplenic
Gastrohepatic
Paracolic gutters
Pouch of Douglas

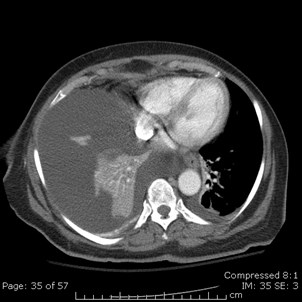

Ascites or Pleural Effusion?
Sharpness of border with liver or spleen
Location of diaphragm
Bare area of liver



Breakdown of smallbowel anastomosis
Abscesses in pouches ofMorison and Douglas


History of Breast Carcinoma
R SubHep
L SubHep



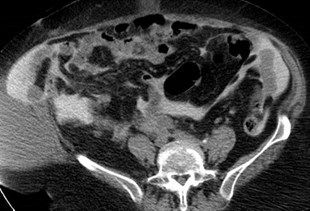
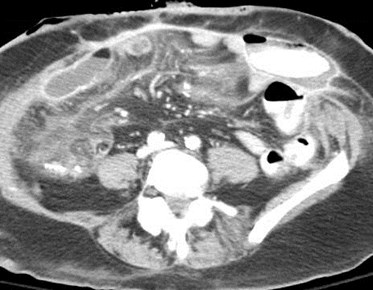
Malignant Ascites: loculated fluid,thickened nodular omentum, nodularthickening in leaves of mesentery


M
a
l
i
g
n
a
n
t
A
s
c
i
t
e
s
:
“
s
t
u
c
k
b
o
w
e
l
”
a
n
d
i
n
f
i
l
t
r
a
t
i
o
n
o
f
o
m
e
n
t
u
m


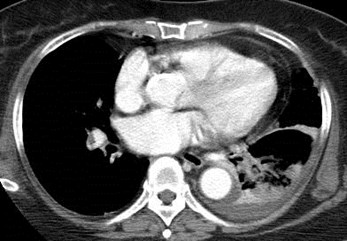



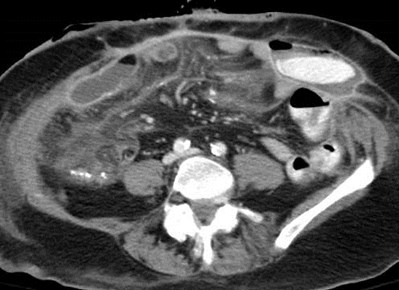
Gastric Carcinoma
pulmonary embolism and peritonealspread with drop metastases

Gastric Carcinoma spreadingvia transverse mesocolon
Ovarian Carcinoma: peritoneal implants





Ovarian Carcinoma withperitoneal metastases
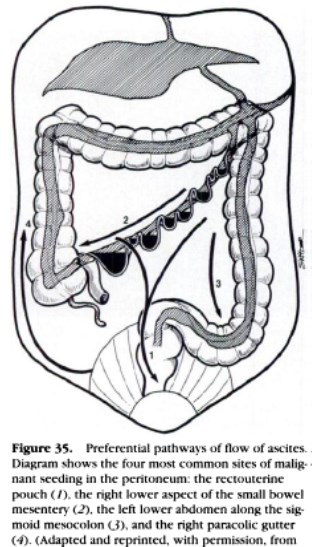
Pathways of Tumor Spread withinPeritoneum
•Direct spread along mesenteric vesselsand surrounding fat
•Extension via mesenteric lymphatics
•Embolic hematogenous spread
•Intraperitoneal seeding
• Though classification is convenient it is somewhatarbitrary because many neoplasms spread by multipleroutes
Peritoneum: Solid Masses
•Almost all are malignant, vast majority aresecondary
•Primary Neoplasms: Peritoneal Mesothelioma,presenting with nodular peritoneal or omentalmasses which may merge to become confluent
•Secondary Neoplasms: Peritoneal CarcinomatosisMost frequent sites: ovary, colon, stomach andother less common sites include pancreas, uterusand bladder
Peritoneal Carcinomatosis
•Ascites, often loculated and not in most dependentspaces
•With IV contrast- enhancement and thickening ofperitoneum
•Calcified metastatic implants may be seen withserous cystadenocarcinoma of ovary
•Thickening and nodularity along leaves ofmesentery, often with encasement of vessels
Embolic Hematogenous Spread
•Tumors: Melanoma, breast, lung cancer
•Reach anti-mesenteric border of smallintestine through small mesenteric arterialbranches.
•Tumor deposits can act as lead point forintussusception.



Metastatic Melanoma: small bowel metastaseswith intussusception, subcutaneous metastases


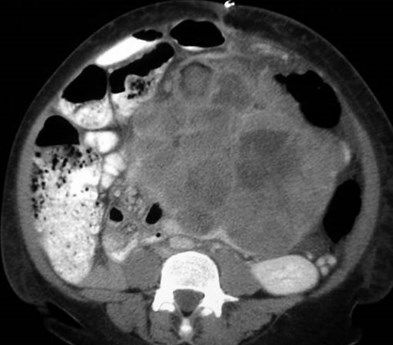
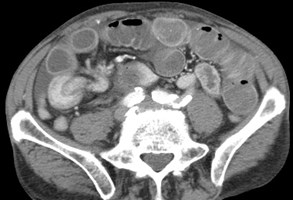
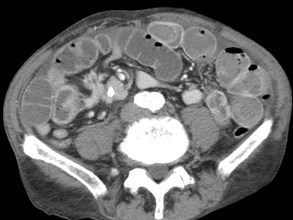
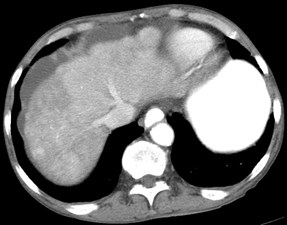
History of mucinous colon carcinoma

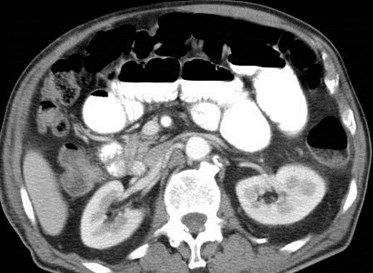
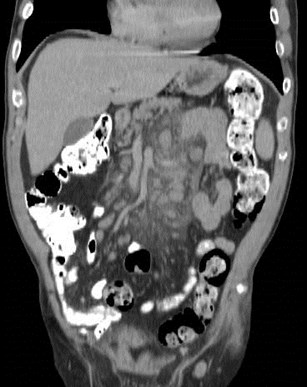
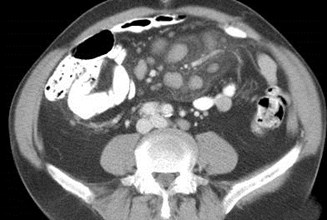
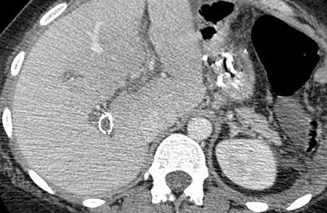
Pseudomyxoma Peritonei
•Clinical findings of slowly increasing abdominalgirth
•CT: heterogeneous peritoneal locules of fluidwhich displace and distort bowel. Characteristicfinding of a scalloped effect on solid organs,sometimes with linear or punctate calcifications
•Due to prior mucocele rupture or transmuralspread of mucinous tumors from appendix,ovary, pancreas, stomach, colon or urachus
Radiographics 2007;27:707


Tuberculous Peritonitis
•CT: Smooth peritoneum with minimal thickening,marked enhancment. Peritoneal andextraperitoneal masses and adenopathy withlow density, calcifications, splenomegaly
•Three forms
–Wet type (most common) with large amounts of freeor loculated viscous fluid with higher than waterdensity due to protein and cells
–Fibrotic fixed type with large omental masses, mattedfixed bowel and mesentery
–Dry plastic type (least common), caseous nodules,fibrous peritoneal reaction, dense adhesions, mostsimilar to peritoneal carcinomatosis or mesothelioma
AJR 1997;168:1455



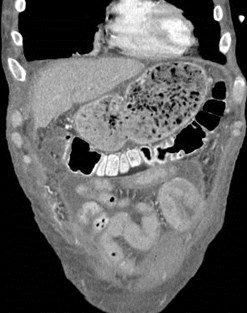
Abdominal Cocoon(sclerosing encapsulating peritonitis)
•Clustering of small bowel loops encased in athin walled sac
•Other CT findings include: SBO, fixation ofbowel loops, ascites, localized fluid collections,peritoneal thickening with enhancement,reactive adenopathy
•May be very difficult to diagnosis when cocooncontains only bowel and no fluid
•Often no precipitating cause
Hur etal. AJR 2004;182:639-641
Gupta etal AJR 2004;183:1658-1660

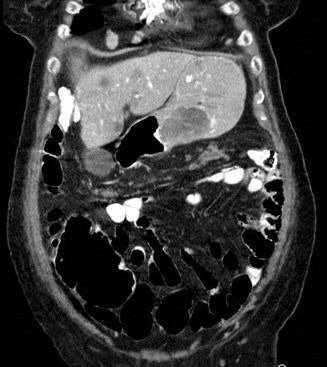
Gastrointestinal Stromal Tumorarising in mesentery
GIST
•Spindle cell, mesenchymal tumors of the gastrointestinaltract
•Spectrum from benign to malignant based upon numberof mitoses
•Typically originate from stomach (more benign) andsmall bowel with 10% from mesentery
•Characterized by well circumscribed tumors, oftenarising in exophytic fashion from stomach or small bowelwith heterogeneously enhancing rim and necrotic center
•Metastases usually to liver and peritoneum
Radiology 2003;226:527


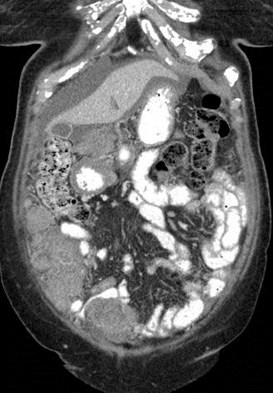
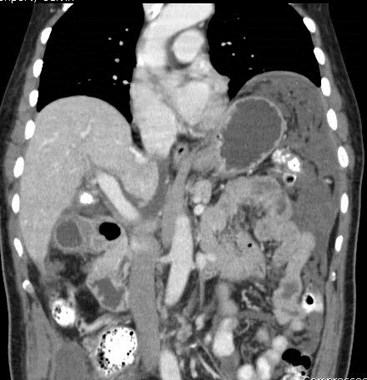
Carcinoid of distal ileum withspread to peritoneum
•Tumors arise from neuroendocrine cells of intestinalmucosa or submucosa
•Most common malignant neoplasm of small intestine
•40 – 80% of GI carcinoids spread to mesentery directlyor through local lymphatics
•Distal ileum is most frequent primary location
•Mesenteric mass is often detected first
•With hepatic metastases, may present with carcinoidsyndrome caused by release of vasoactive substances(flushing, wheezing, right-sided heart failure caused bystenosis of tricuspid and/or pulmonic valves)
Carcinoid of distal ileum withspread to peritoneum
•Most common CT manifestation is enhancing softtissue mass with linear bands radiating intomesenteric fat
•Radiating strands not usually tumor, but due tointense desmoplastic reaction caused by releaseof serotonin and other substances
•Calcifications occur in 70%
•Thickening of adjacent small bowel loops causedby tumor infiltration or ischemia from sclerosis ofmesenteric vessels with angulation
•Liver metastases best visualized in arterial phase
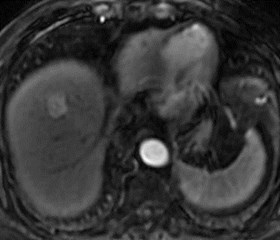
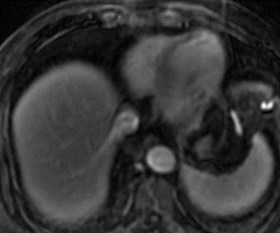
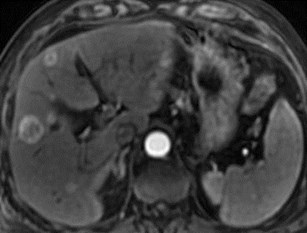
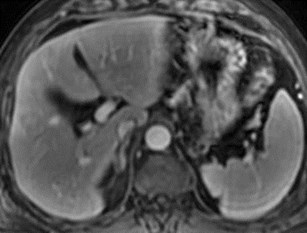
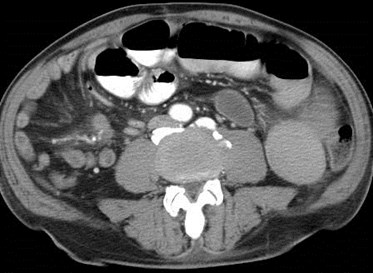
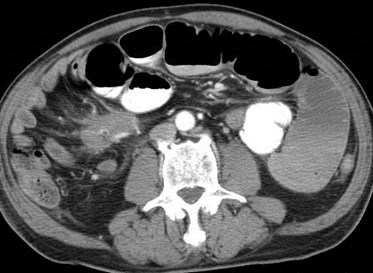
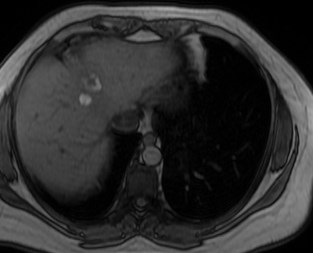
Carcinoid in small bowelmesentery with intussusceptionand liver metastases causingpseudo-cirrhosis


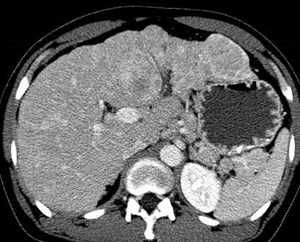
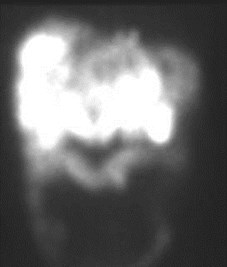
Metastatic carcinoid to liver causing “pseudo-cirrhosis” positive octreatide scan
Immediate
Delayed
Metastatic Carcinoid- liver metastases witharterial phase enhancement



3-06
11-06
5-07
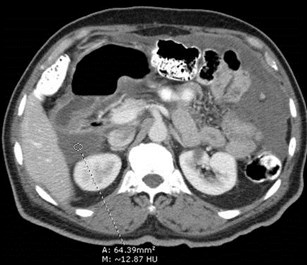
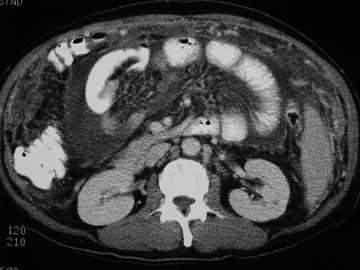
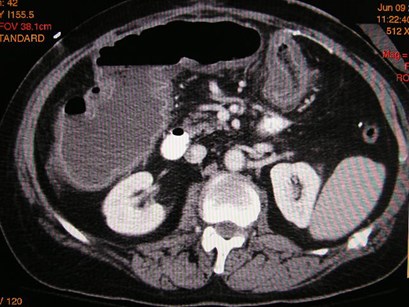
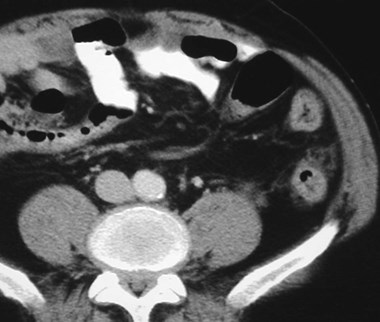
Mesenteric Panniculitis


Mesenteric Panniculitis

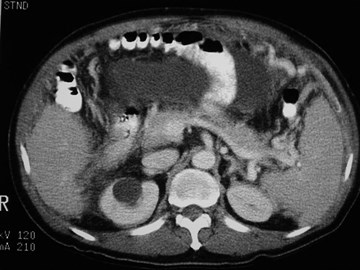
Retractile mesenteritis with SBO
Sclerosing Mesenteritis
•Synonyms: retractile mesenteritis, systemicnodular panniculitis, liposclerotic mesenteritis,xanthgranulomatous mesenteritis
•Differential Diagnosis: inflammatory pseudotumor,desmoid tumor, carcinoid, mesentericmetastases, lymphoma
•3 Subgroups based upon predominant tissue type
–Mesenteric panniculitis: characterized by chronicinflammation
–Mesenteric lipodystrophy: fat necrosis
–Retractile mesenteritis: fibrosis
Radiographics 2003;23:1561
Sclerosing Mesenteritis
•Rare condition of unknown cause
•Usually involves root of small bowel mesentery,but can also involve mesocolon
•Often associated with other idiopathicinflammatory disorders including retroperitonealfibrosis, sclerosing cholangitis, Riedel thyroiditisand orbital pseudotumor
•Clinical: abdominal pain, intestinal obstruction orischemia, mass, diarrhea. Male predilection,middle age
Retractile Mesenteritis
•Soft tissue mass in small bowel mesentery
•Mass may envelope and occlude vessels withdevelopment of collaterals
•Calcification is common in central necrotic portionof mass. Cystic components andlymphadenopathy may develop.
•Biopsy is necessary for diagnosis, especially todifferentiate from carcinoid and other tumors.
Misty Mesentery
•Definition: Increased attenuation of smallbowel mesentery at CT
•Mesenteric Panniculitis: characterized by“fat ring” sign and “tumoralpseudocapsule”
•Other causes: Edema, malignancy,inflammation/fibrosis
Radiology 2003;226:86
AJR 1996;167:61

Lymphoma



Mesenteric and Portal Thrombosis
Recent gastric bypass


Bladder Cancer metastaticto peritoneum

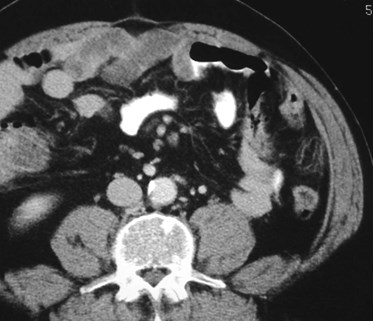
16 year old with right lowerquadrant pain
Mesenteric Adenitis
Interloop Abscesses
Fat Necrosis in Omentum


Ischemic Colon
Post-op
Fat Necrosis
Epiploic Appendagitis
Fat Infarction: Omentum, EpiploicAppendages
•Idiopathic, 2° surgery
•Usually self limited, but occasionally maybecome infected
Miscellaneous



Thickening of colon with associated inflammatory mass
History of fever and pain
Actinomycosis
•2° Actinomycoses israelii, a gram positive anaerobepresent in normal oral cavity, considered opportunistic,usually following a perforated viscus, surgery, trauma orlong term use of intrauterine contraceptive device
•Characterized by multiple abscesses, draining sinuses,granulation and fibrotic tisse
•A chronic, progressive, suppurative disease
•GI involvement most common in colon with concentricwall thickening and large “mass” adjacent to bowel,often extending through compartments to skin surface.Distinctive lack of diffuse peritoneal spread of ascites.
Radiology 2002;220:76



Inguinal Hernia Repair
•Focal pelvic lesions very common (almost 90%) in thosewith plug mesh repair (more common than with flat meshrepairs)
•CT finding probably represents a combination of trappedfluid, old blood or scar tissue
•Typically ovoid in shape, deep to internal inguinal ring
•Maximum mean diameter 2.4 cm (range 1.3 – 3.9 cm)
•Mean attenuation 17 H.U. (range -4 to 64 H.U.)
•May be mistaken for lymph node
Chernyak, etal. JCAT 2007;31:724
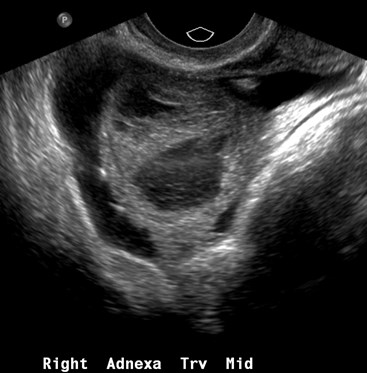
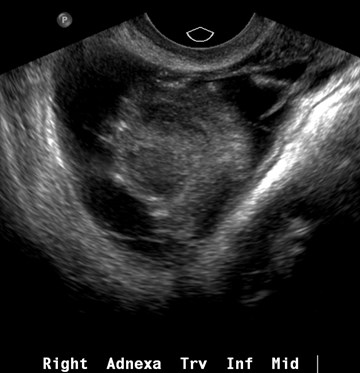
Peritoneal Inclusion Cyst
History of pelvic inflammatory disease
Peritoneal Inclusion Cyst
•Requires active ovary and peritoneal adhesions
•Formed of non neoplastic mesothelial proliferation, “benigncystic mesotheliomas”
•Appear as complex, multicystic adnexal masses adherentsurface of ovary
–Can simulate neoplasm, hydrosalpinx, paraovarian cyst
•History of surgery, trauma ,infection, endometriosis
•Patients present with pain and/or mass
•Treatment: oral contraceptives, pain meds, aspiration
Jain. AJR. 2000;174:1559

Three young women with same diagnosis
1
2
3
Endometriosis
•Proposed Theories
–Metastatic implantation from retrograde menstruation
–Metaplastic differentiation of serosal surfaces or mullerioanremnant tissues
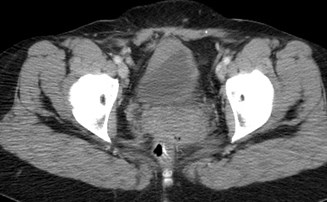
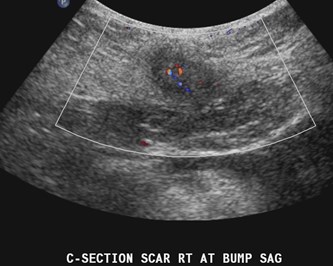
•Unusual Locations
–Scars, particularly from Cesarean section
–Round ligament, hernia sacs, skin
–Urinary tract, particularly bladder
–Bowel: rectosigmoid, appendix, cecum, small bowel
Choudhary, etal. AJR 2009;192:1632
Hensen, etal. AJR 2006;186:616
THE END


Hawaii February, 2013