Abdominal andPelvic Hernias
SLS 4/2004
Images from
Textbook of Gastrointestinal Radiology,
Gore, Levine, Laufer
And Drawings from Netter
Abdominal and Pelvic Hernias
Internal hernia
External hernia
Diaphragmatic hernia
Internal Hernias
Protrusion of organs or parts thereof,through an abnormal opening, fromtheir natural place in a cavity
Internal Hernias
Autopsy incidence <1%
May remain clinically silent if easilyreducible
Larger ones symptomatic
Vague epigastric discomfort
Colicky periumbilical pain
Recurrent episodes of intestinal obstruction
Internal Hernia
Physical examination
May reveal palpable mass of herniated bowel loops withlocalized tenderness
Diagnostic studies (BE, fluoro) most helpful duringsymptomatic period
Otherwise, hernia may not be recognized once it is reducedspontaneously or if decompressed by NG tube.
If incarcerated, most common presentation isacute SBO
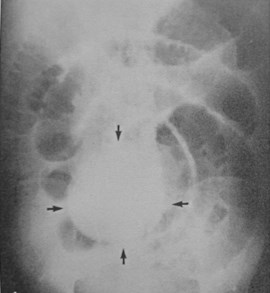
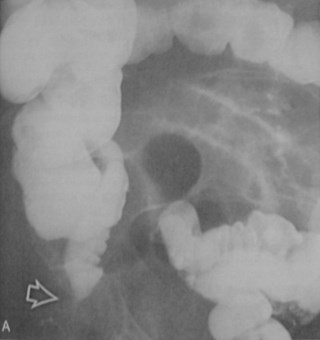
Barium and CT findings in internalhernias
1 Abnormal location of intestinal segment
2 Encapsulation and crowding together of SBloops in the confines of peritoneal cavity
3 Stasis of contrast material in lumen and dilationof proximal bowel
4 Apparent fixation of herniated loops, notseparable during fluoro or changes in patientposition
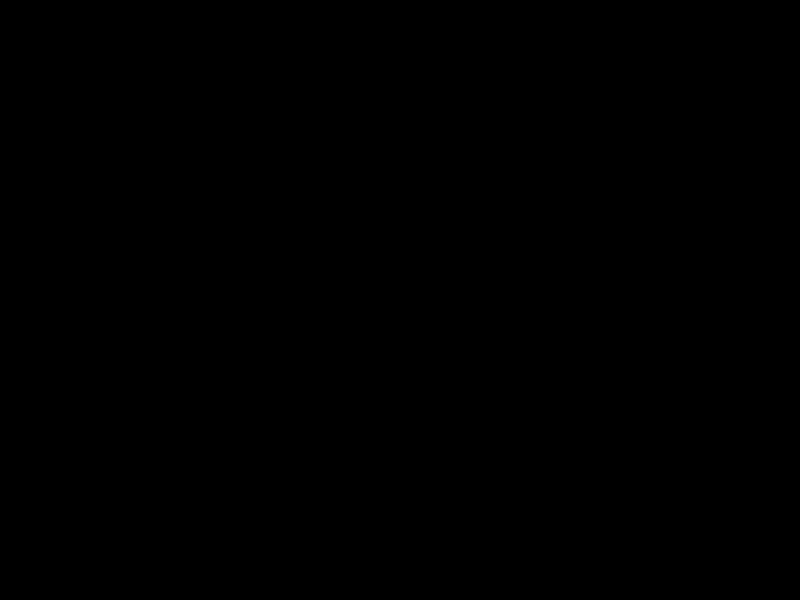
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
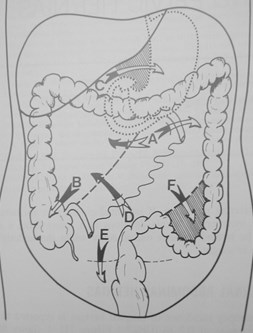
Paraduodenal Hernia
Most common type of intraabdominalhernia
Men>women {3:1}
Left>right {75%}
Paraduodenal hernias
Left
Through fossa of Landzert into descendingmesocolon
Right
Through fossa of Waldeyer into ascending ortransverse mesocolon
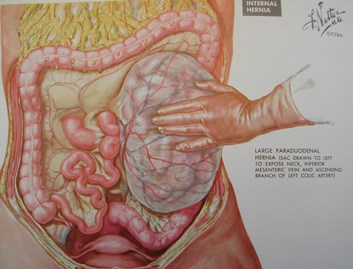
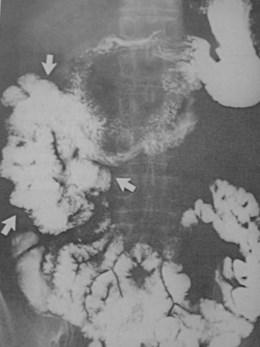
Left Paraduodenal Hernia
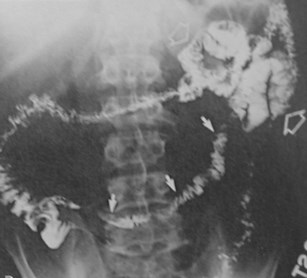
Left-sided paraduodenal hernias
Mass of barium-filleddilated small bowel loops inLUQ, lateral to 4th portion ofduodenum
Lateral to descending colon
On lateral view, appearsretroperitoneal
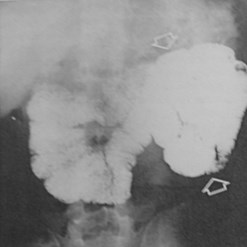
Left paraduodenal hernia
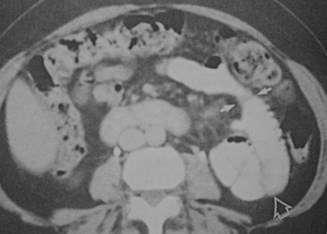
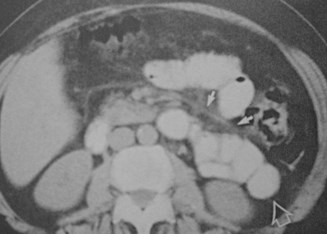
Right sided paraduodenal hernias
Mass of small bowel loops lateral andinferior to 2nd part of duodenum
Bowel passes into the ascending andtransverse mesocolon
Lateral view- hernia contents inretroperitoneum
Right paraduodenal hernia
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
Foramen of Winslow hernia
Hernia contents extendinto lesser sac
Contents include smallbowel, cecum, GB, TI,ascending or transversecolon
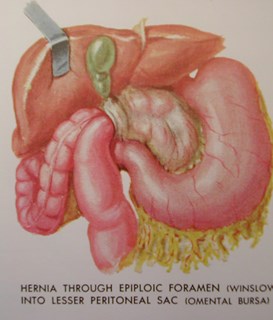
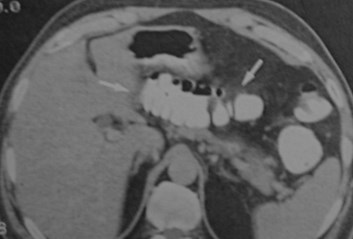
Foramen of Winslow hernia
Radiographic findings
Gas-containing bowel in lesser sac medial andposterior to stomach
Dilated proximal bowel
Displacement of stomach anteriorly and to the left
Foramen of Winslow hernia


Foramen of Winslow Hernia
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
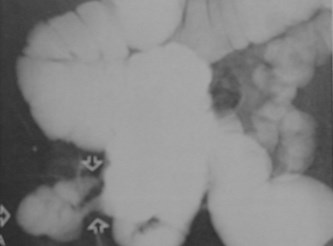
Pericecal Hernias
Ileal loop pushes through defect in cecalmesentery
Loop then seen in right paracolic gutter
Symptoms
Colicky RLQ pain
Can mimic appendicitis


Pericecal hernia
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
Intersigmoid Hernia
Ileal or jejunal loopsinterposed betweentwo sigmoid loops


Intersigmoid hernia
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
Transmesenteric Hernia
Through defects in mesentery of smallbowel
Results in closed loop obstruction

Transmesenteric hernia

Transmesenteric hernia
Leftcolon
Small bowelin hernia sac
Internal Abdominal Hernia
Paraduodenal
Foramen of Winslow
Pericecal
Intersigmoid
Transmesenteric
Retroanastomotic
Retroanastomotic Hernia
Complication of GI surgery- usually afterpartial gastrectomy and gastrojejunostomy
Usually incarceration of the efferent jejunalsegment in retroanastomotic space

Retroanastomotic hernia afterBillroth II gastrojejunostomy
Efferent loop
Afferentloop
External Abdominal Wall Hernias
Protrusion ofabdominal contentsthrough an abdominalwall defect
Umbilical
Ventral
Spigelian
Lumbar
Incisional
External Abdominal Wall Hernias
Umbilical
Ventral
Spigelian
Lumbar
Incisional
Umbilical Hernia
In infants and children, due to patentumbilical ring
In adults, usually women with obesity ormultiple prior pregnancies
Incarcerated umbilical hernia

External Abdominal Wall Hernias
Umbilical
Ventral
Spigelian
Lumbar
Incisional

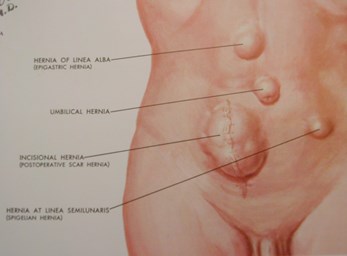
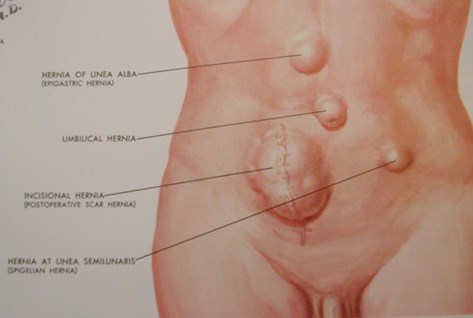
Ventral Hernias
Usually throughdefect in aponeurosisthat forms linea alba
Epigastric
Superior to umbilicus
More common
Hypogastric
Inferior to umbilicus
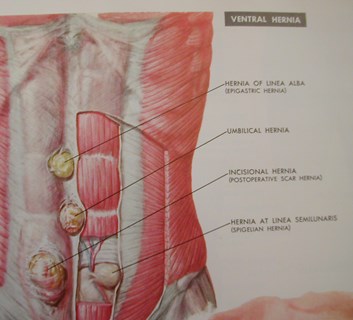
Ventral Hernia
External Abdominal Wall Hernias
Umbilical
Ventral
Spigelian
Lumbar
Incisional
Spigelian Hernia
Anterolateral lower abdominal wall,along semilunar line
Fibrous union of rectus sheath withaponeuroses of transversus abdominisand oblique abdominal muscles
Spigelian Hernia
External Abdominal Wall Hernias
Umbilical
Ventral
Spigelian
Lumbar
Incisional
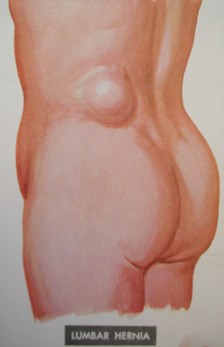
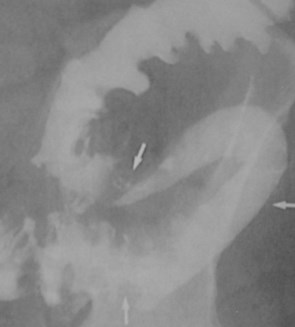
Lumbar Hernia
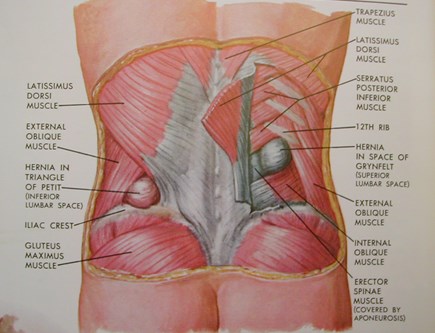
Lumbar Hernia
Superior lumbar space ofGrynfeltt-Lesshaft
Inverted triangle boundedby 12th rib superiorly,internal oblique muscleanteriorly, erector spinusmuscle posteriorly
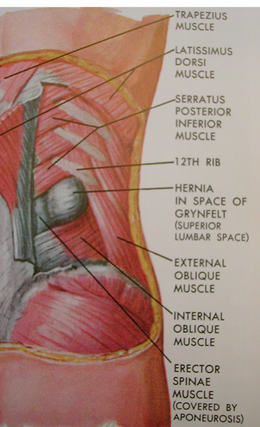
Lumbar Hernia
Inferior lumbarspace-Petit’s triangle
Bordered inferiorly byiliac crest, anteriorly byexternal obliquemuscle, posteriorly bylatissimus dorsi
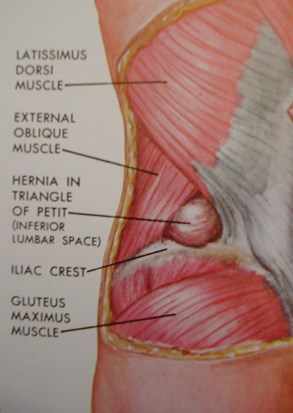

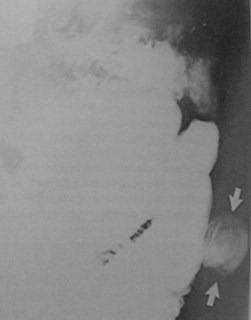
Lumbar hernia
External Abdominal Wall Hernias
Umbilical
Ventral
Spigelian
Lumbar
Incisional
Incisional Hernia
Usually occur within first 4 months aftersurgery
Occur in up to 5% of patients
Contents
Properitoneal fat, omentum, and eventually bowel

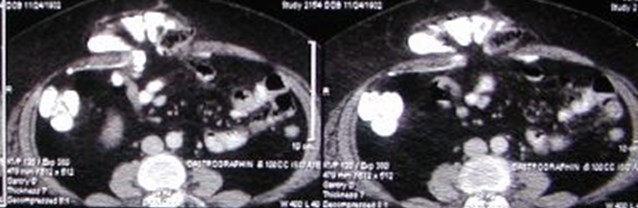
Large paraileostomy hernia

Incisional Hernia

Incarcerated incisional hernia
Pelvic Wall and Groin Hernias
Inguinal
Femoral
Obturator
Sciatic
Perineal
Inguinal Hernia
Indirect
Lateral to inferior epigastric vessels
Most common type
Direct
Protrudes directly through lower abdominal wallmedial to inferior epigastric vessels
Indirect Inguinal Hernia
Congenital
Failure of peritoneal sac (processus vaginalis) toobliterate
Bowel protrudes through inguinal canal and exitsat external inguinal ring
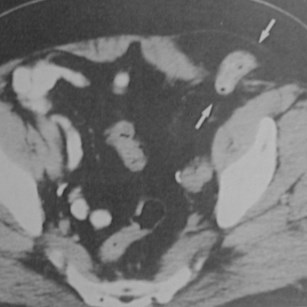
Indirect inguinal hernia
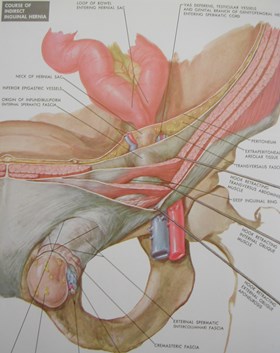


Indirect inguinal hernias


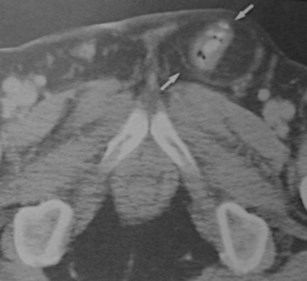
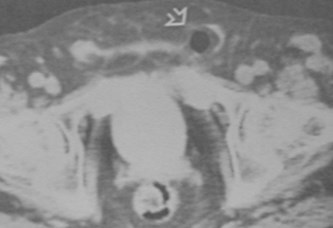
Inguinal Hernia on CT
Direct Inguinal Hernia
Rare in children
40 – 50 years of age
Male> Female
Predisposing factor isweakness at inguinaltriangle (Hesselbach’s)
Medial to inferiorepigastric vessels
Hesselbach’s triangle
Medial boundary:Rectus abdominis
Lateral boundary:Inferior epigastricvessels
Inferior boundary:Inguinal ligament
Pelvic Wall and Groin Hernias
Inguinal
Femoral
Obturator
Sciatic
Perineal
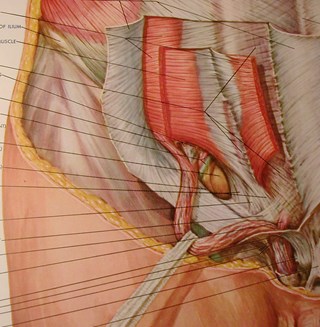
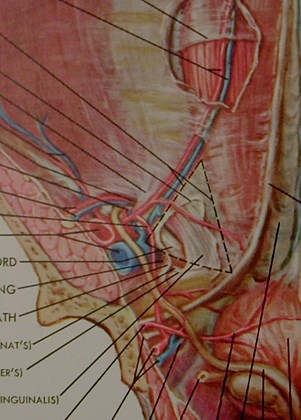
Femoral Hernia
Deep to femoral canal
Difficult to diagnose clinically
Contents – omentum, SB
Below inguinal ligament
Prone to incarcerate
Women>Men
Right > Left (3:1)
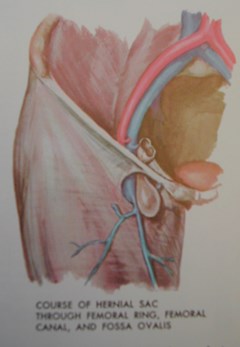
Femoral Hernia
Femoral and Inguinal Hernias
Femoral
Inguinal
Pelvic Wall and Groin Hernias
Inguinal
Femoral
Obturator
Sciatic
Perineal
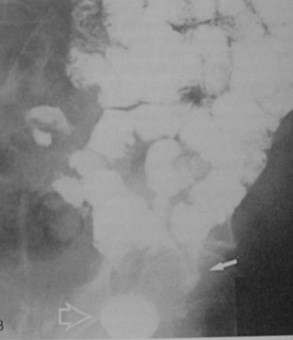
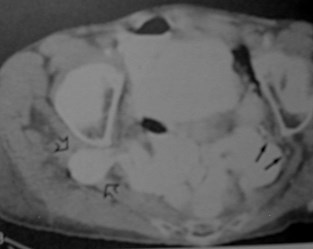
Obturator Hernia
Through obturator canal in superolateralaspect of obturator foramen
Between pectineal and obturator muscles
Usually elderly women
Contain bowel, appendix, omentum,bladder or uterus
Typically incarcerates
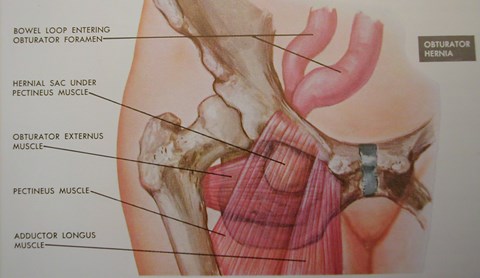
Obturator Hernia
Pelvic Wall and Groin Hernias
Inguinal
Femoral
Obturator
Sciatic
Perineal
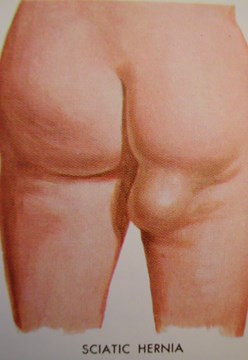
Sciatic Hernia
Through greater or lessersciatic notch
Under inferior border ofgluteus maximus andabove or below piriformismuscle
Presents in posteromedialaspect of thigh
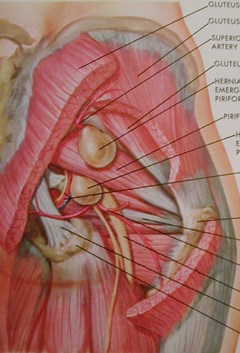
Sciaticnerve
Gluteusmax.
piriformispiriformis
Sciatic Hernia
Contains distal ureter or small bowel
Strangulation of hernia contents occursfrequently
May present with bowel obstruction
May present with pain along distribution ofsciatic nerve
Incarcerated Sciatic Hernia
Pelvic Wall and Groin Hernias
Inguinal
Femoral
Obturator
Sciatic
Perineal
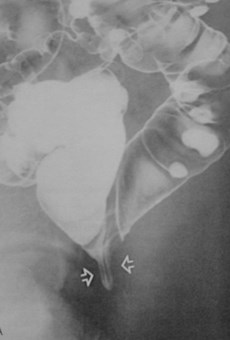
Perineal Hernia
Occur at weak areas of UG diaphragm,levator ani, or coccygeal muscle
Present as perineal or gluteal mass
Barium studies or CT
Depict bowel ischiorectal fossa, labia majora orin the buttock
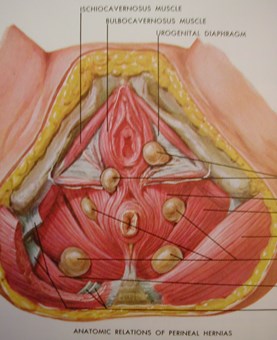
Perineal Hernia
Other Hernias…
Richter’s Hernia
Involves only part of the bowel wallcircumference
Usually no obstructive symptoms, but painfrom incarceration of involved segment
Richter’s Hernia
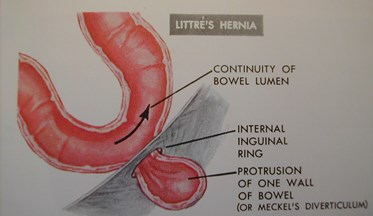
Littre’s hernia
Meckel diverticulum protrudes into hernia sac
Usually occurs in right inguinal region

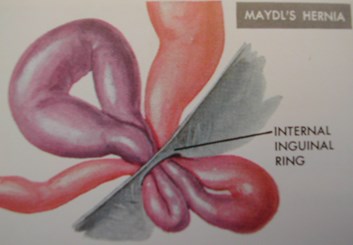
Maydl’s hernia (hernia in W
very rare
contains two loops ofbowel arranged like a 'W’
central loop of 'W' lies freein the abdomen and isstrangulated whereas thetwo loops present in thesac often are not
Garengoff’s hernia
Hernia sac has the appendix

Pantaloon Hernia
Concurrent direct and indirect inguinalhernias
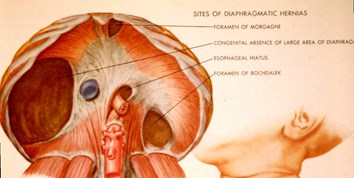
Diaphragmatic Hernias
Protrusion of abdominal contents into thechest
Esophageal hiatus
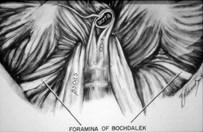
Foramen of Bochdalek
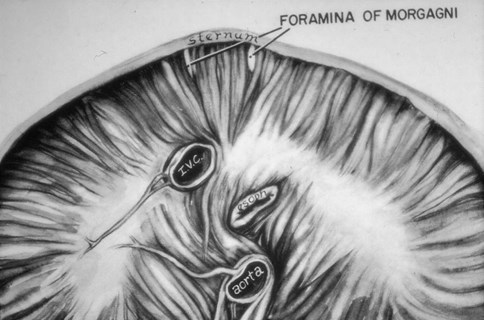
Foramen of Morgagni
Acquired defectgs
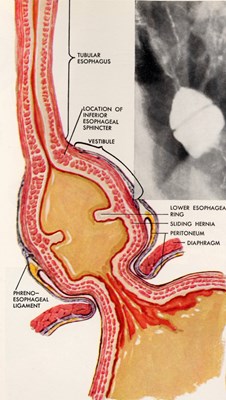
Esophageal hiatus
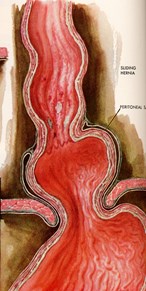
Sliding HH
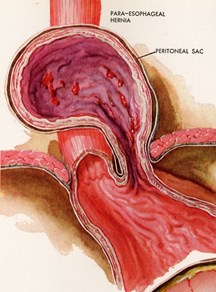
Paraesophageal hernia
Sliding hiatal hernia
Common10% of adults
Due to weakening of phrenicoesophagealmembrane
EG junction above diaphragm
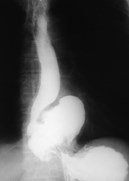
Paraesophageal hernias
Stomach protrudes through esophagealhiatus parallel with distal esophagus
EG junction remains below diaphragm
Complications
Incarceration, strangulation, infarction
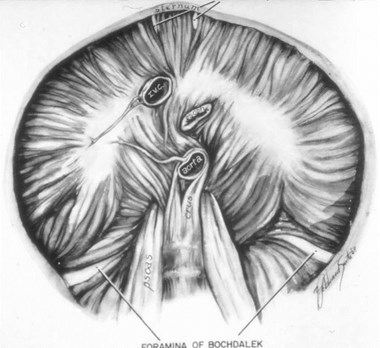
Bochdalek Hernia
Posterolateral
Congenital
Abnormal development of diaphragm
Acquired
Surgery, trauma, infection
Morgagni Hernia
Anterior, Midline
Acquired diaphragmatic hernia
Penetrating or blunt trauma
Increased intraabdominal pressure
Ant-R
Post-L
Foramina ofMorgagni
IVC
Foramina of Bochdalek
Aorta
Esophagus
Diaphragmatic HerniasTypes of
Congenital
Bochdalek
Morgagni
Traumatic
Hiatal
Congenital Diaphragmatic HerniasGeneral
Absence of closure of pleuroperitoneal fold
9th gestational week
Male:female ratio of 2:1
1:2,000 live births
Left > right 9:1
Bochdalek HerniaGeneral
90% of congenital hernias
Posterolateral defect
Abnormality of cephalic fold ofpleuroperitoneal membrane
Left (80%) > right (15%) > B/L(5%)
Babies – large defect
Adults – small small defect
Bochdalek HerniaOrgans Involved
Bowel
Spleen
Fat
Liver (left lobe)
Kidney, pancreas
Stomach
Bochdalekherniacontaining leftkidney

Large Bochdalek Hernia


Bochdalek HerniaThe “B’s”
Babies
Back
Big
Morgagni HerniaGeneral
Anteromedial parasternal defect(Space of Larrey)
Maldevelopment of septum transversum
Overweight, middle-aged, women
Right > left (heart protects)
Associated with
Pericardial defects
Omental fat in pericardial space
Ant
Foramina of Morgagni
Morgagni HerniaOrgans Involved
Liver
Bowel
Morgagni HerniaThe “M’s”
Middle (anterior and central)
Mature (older children)
Miniscule
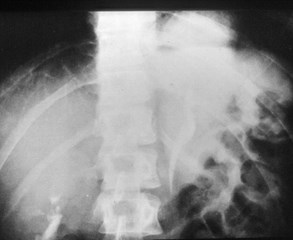
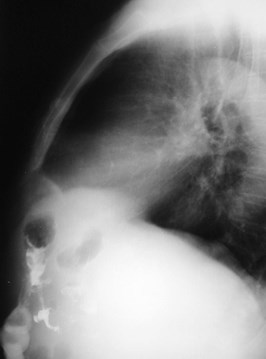
Congenital Diaphragmatic HerniaX-ray Appearance
Bowel loops in chest
Transverse colon peaks anteriorly in Morgagni
Contralateral shift of heart/mediastinum
Scaphoid abdomen
Polyhydramnios on US
Colon in Morgagni Hernia

Traumatic Diaphragmatic HerniaGeneral
5% of all diaphragmatic hernias
90% of all strangulated hernias
Contain stomach, colon, small bowel,omentum, spleen
May be asymptomatic for months oryears following injury
Left (90–98%) > right (2–10%)
Central and posterior
>10cm in length
Associated with
Fx ribs
Pneumoperitoneum
Ruptured spleen
Traumatic Diaphragmatic HerniaGeneral
Traumatic Diaphragmatic HerniaEtiology
Blunt trauma (5–50%)
2° increased intra-abdominal pressure
MVA, fall from height
Penetrating trauma (50%)
Knife, bullet
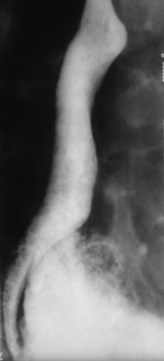
Hourglass Configuration

Characteristic of hernia
Rupture Left Hemidiaphragm
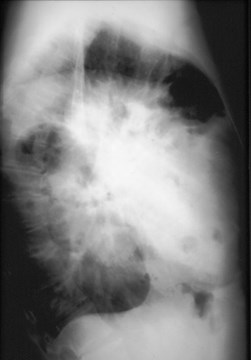

Rupture Left Hemidiaphragm

Traumatic Diaphragmatic HerniaComplications
Hydrothorax
Hemothorax
2° strangulation
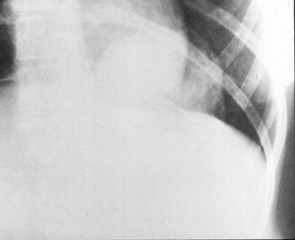
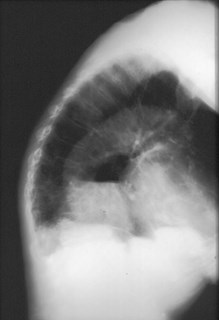
Hiatal HerniaGeneral
Most common form of diaphragmatichernia in adult
Air/fluid level(s) in “mass” posterior toheart
May contain entire stomach which canvolvulate
Large Hiatal Hernia

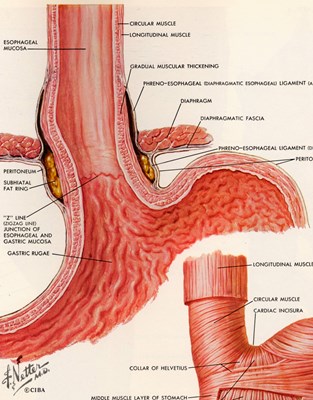
A =contractilering
Phrenicampulla
“Z line” =EG junction
Normal EG Junction
Normal versus Hiatal Hernia
Hiatal HerniaTypes
Sliding
EG junction above diaphragm
Para-esophageal
EG junction below diaphragm
Paraesophageal
Sliding

Paraesophageal
Sliding

Hiatal HerniaTypes
Reducible
EG junction sometimes below diaphragm
“Sliding” mistakenly used to meanreducible
Incarcerated
EG junction (hernia) stay abovediaphragm
Hiatal HerniaA Ring and B Ring
A ring
Contractile ring
Dynamic
B ring
Static ring
EG junction
Hiatal HerniaAnti-reflux Mechanisms
Normal stomach
EG junction
A ring
Cricopharyngeal muscle
Abnormal stomach
Paraesophageal hiatal hernia
Large hiatal hernia
“A’ contractile,dynamic ringacts to stopreflux
“B” static ring(Schatzki’sring) is the EGjunction
Phrenic ampulla- normal
A and B Rings
A Ring
B Ring


Hiatal HerniaReflux
Hiatal hernia predisposes to reflux
Reflux can occur without HH
Patulous cardia
Esophagus should narrow to 50%tubular diameter passing throughdiaphragm
If not to reflux

As esophaguspasses throughdiaphragm, itdoes not narrowto 50% diameterof tubularesophagus