
CT of Urinary Trauma
Mindy M. Horrow, MD, FACR, FSRU
July 15, 2013
Director of Body Imaging, Einstein Medical Center
Professor of Radiology, Jefferson Medical College
Etiology
Blunt trauma accounts 80%–90% of all cases, withmotor vehicle accidents being most common cause
Gunshot wounds may cause blast affect withcavitation and necrosis
less common causes include
–(a) direct blow to flank or abdomen during anassault, fight, sports activity (eg, bicycling,horseback riding)
–(b) fall from a height.
Alonso, etal. RadioGraphics 2009; 29:2033–2053
CT of Renal Trauma
Injury is common but 95% minor
Hematuria in 95% with renal trauma
Renal pedicle or vein injury may have nohematuria
Initial imaging @ 70-80 sec for vascularenhancement and nephrogram
Delayed images (3-5 min) to check for urineleak
American Association of SurgicalTrauma
Grade 1- contusion, subcapsular hematoma
Grade 2- non expanding perirenal hematoma, smalllaceration
Grade 3- renal laceration > 1 cm
Grade 4- renal laceration extending to collecting system,injury involving renal artery or vein with containedhematoma
Grade 5- shattered kidney, UPJ avulsion, vascularavulsion
CT Findings of Renal Injuries
Contusions: patchy areas of decreasedenhancement, striated nephrogram
Lacerations: irregular, linear, low-attenuation
Fracture: a laceration through hilum
Subcapsular hematoma: low attenuationcrescent, compressing parenchyma
Arterial injuries: main, segmental
Venous injuries: persistent nephrogram
Collecting system injuries: initial waterdensity, delayed extravasation dense urine
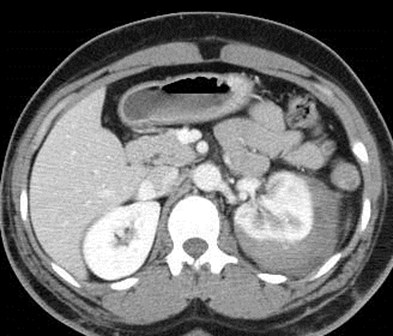

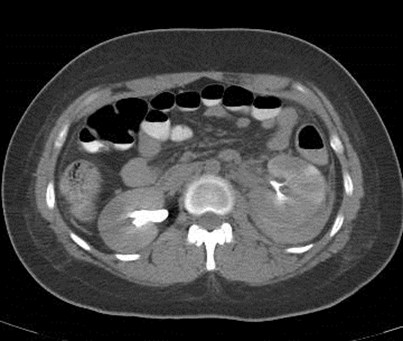
SubcapsularHematoma: Grade 1
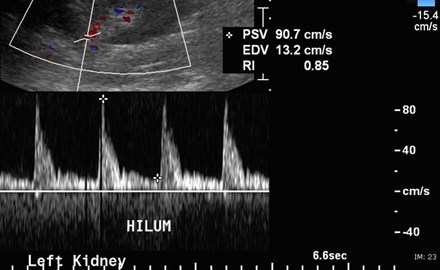
2 days later
Hematoma compresseskidney causing delayednephrogram andelevated resistive index
Initial Delayed
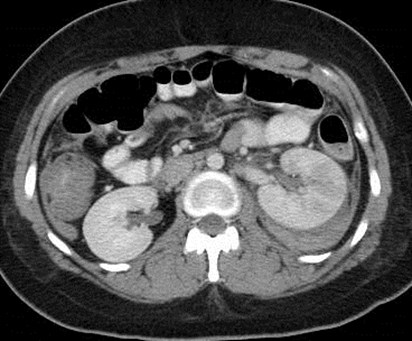
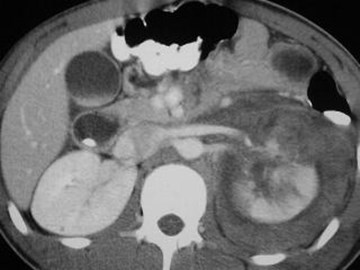
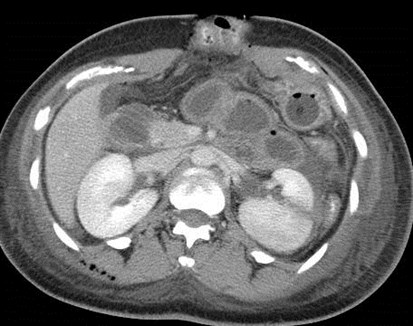
Striated nephrogram, perinephric hematoma
Grade 2 injury


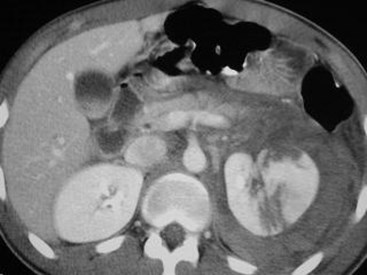
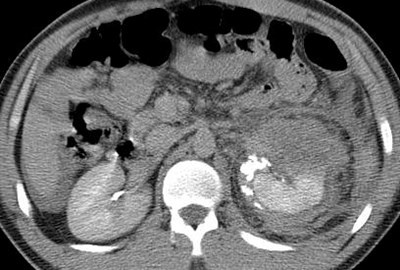
Full thickness laceration, clot in renal pelvisbut no collecting system injury, perinephrichematoma: Grade 3

Initial
Delayed
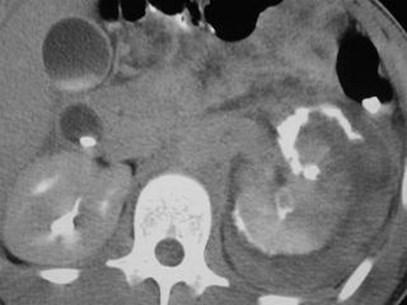
Grade 4:
Laceration of kdney involvingrenal pelvis with urineextravasation and retroperitonealhematoma
Renal lacerations with
hematoma:
initial imaging
Injuries to collectingsystem
with extravasation: Grade 4
Delayed imaging
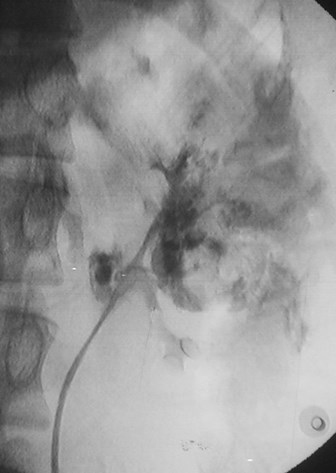

Retrograde study, stent placement


IVU several weeks later with healed,intact collecting system
nephrogram
pyelogram
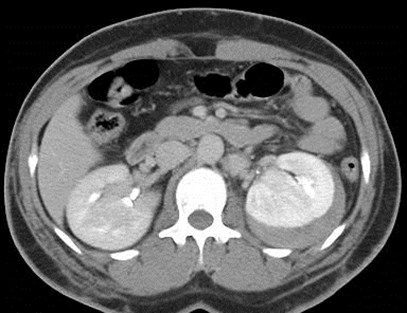
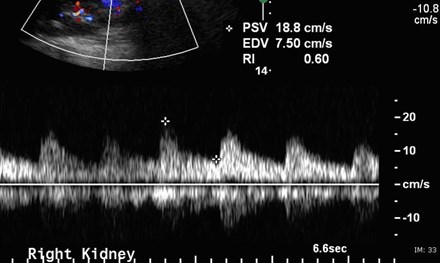
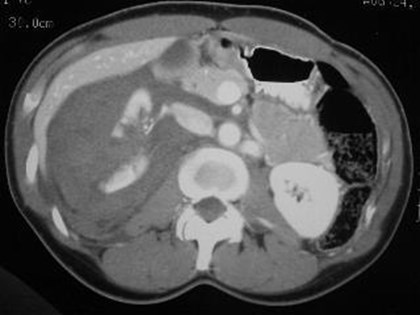
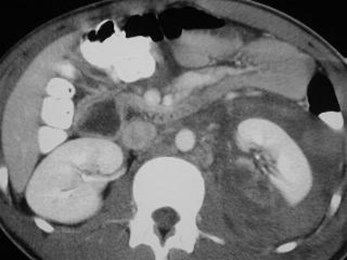
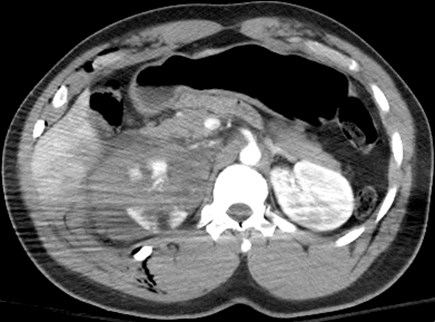
Initial image with slightly delayed left
nephrogram, perinephric fluid andnon occlusive renal vein thrombus

Renal pelvis injury: Grade 4
Delayed imaging

Renal pedicle injury: Grade 5
Non functioning right kidney with injuries to arteryand vein


Post exploratory laparotomy: Early Late
Acute vascular extravasation: Grade 5

Healed spontaneously, mildly delayednephrogram and pyelogram
4 days later

1. Partial main renal arteryinjury
2. Presumed avulsion lowerpole renal artery
3. Collecting System injury
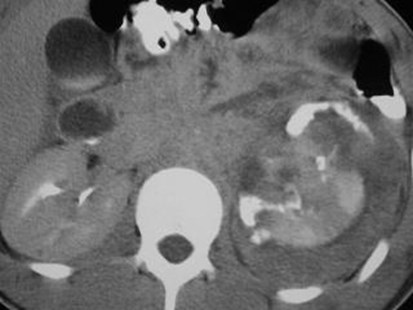
Grade 5




2 months later
Delayed function upper pole, infarctedlower pole with capsular rim sign andretroperitoneal collaterals
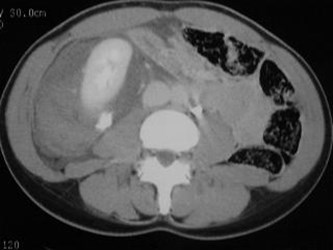
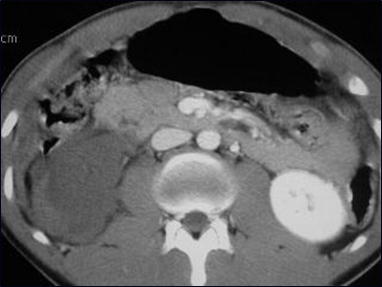
Shattered kidney: Grade 5

Initial study
Trauma related to pre-existing pathology
One day later

Hemorrhageinto cyst
Rupture bilateral renal cysts



Increasing painseveral days later
New Hemorrhage
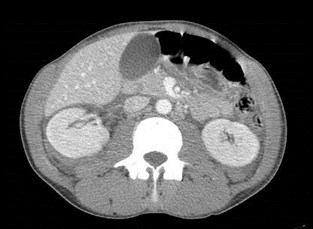
Initial study with renalcontusion

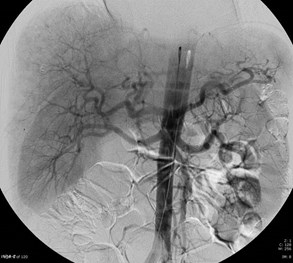
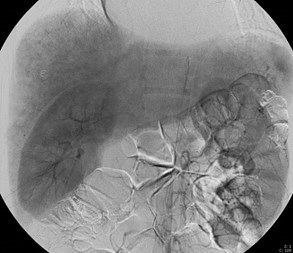

Post traumatic pseudoaneurysm treated with embolization

Initial Delayed

1 week later
2 months later
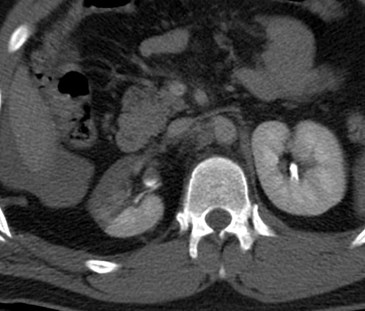
Ureteral injury
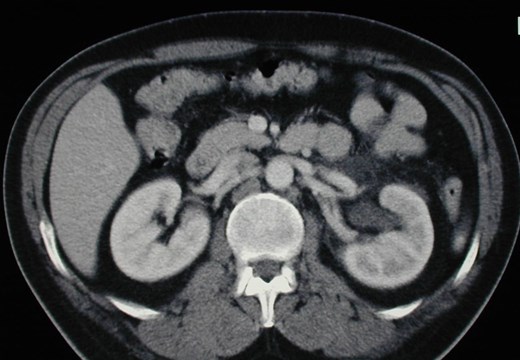
Parenchymal scarring
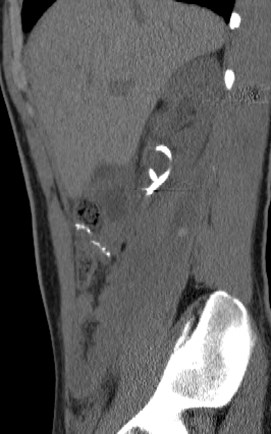
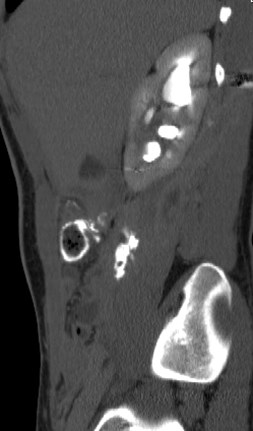

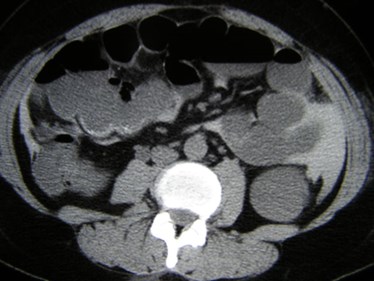
Follow up CT Urogram after renal trauma
Psoas urinoma and uretero-colic fistula
Complications
Occur in 3%–33% of all cases of renal trauma
Early complications develop within first month andinclude urinary extravasation with urinoma formation,infected urinoma, perinephric abscess, sepsis, anddelayed bleeding secondary to arteriovenous fistula orpseudoaneurysm
Late or delayed complications develop more than 4 weeksafter injury and in-clude hypertension, hydronephrosis,calculus and chronic pyelonephritis
Posttraumatic renovascular hypertension may occuranywhere from a few weeks to decades following injury,but on average occurs within 34 months
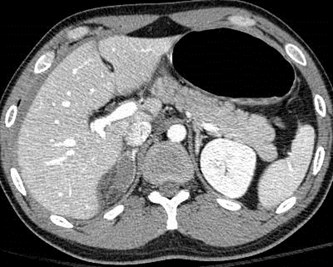

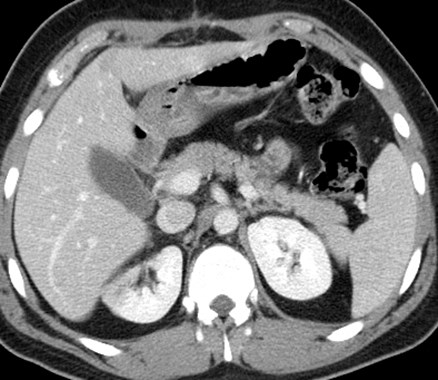
AdrenalHematomas
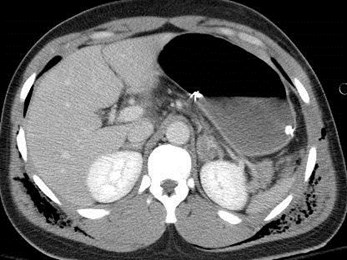
Two different patients
Adrenal Trauma
Adrenal injuries in 1.9% of thoseundergoing CT
Hematoma (obscured gland), activeextravasation
May need follow-up to rule out a trueadrenal mass
These patients had other severe injuriesassociated with a higher mortality
Rana. Rad 2004;230:669-675
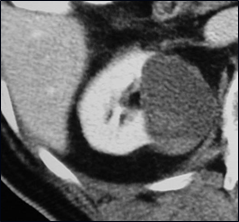
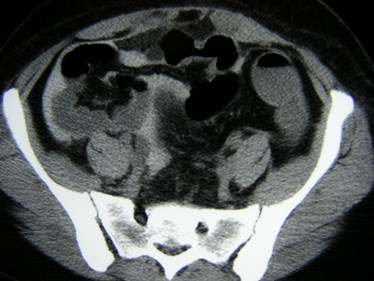
CT of Bladder Injuries
70% associated with pelvic fractures
Add on CT cystogram if bladder isnot distended at time of initial scan
1. ~ 350 mL of 5% contrast materialinstilled via Foley
2. Evaluate urethra before Foleyplacement as necessary
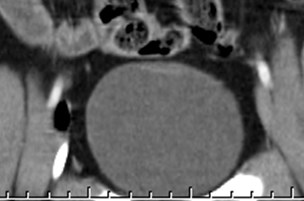
CT Findings of Bladder Injuryon Cystogram
Contusion - focal thickening, variableattenuation
Rupture - extravasation
1.Extraperitoneal - peri/prevesical,anterior abdominal wall, thigh, penis,scrotum
2.Intraperitoneal - pericolic gutters,around bowel loops, pouch of Douglas
No extravasation, minor contusion
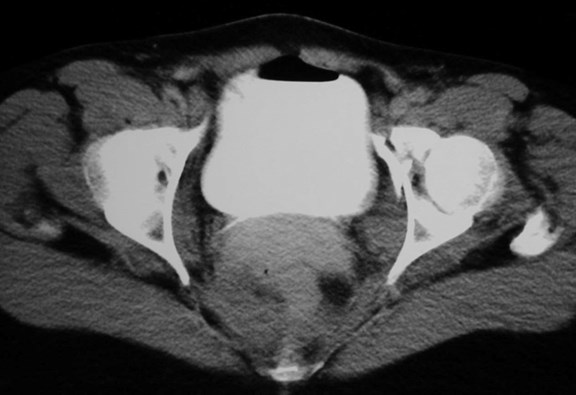
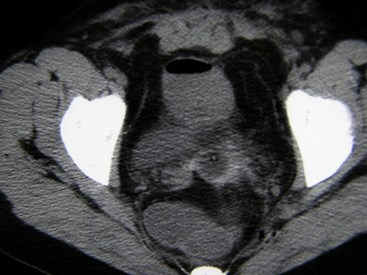
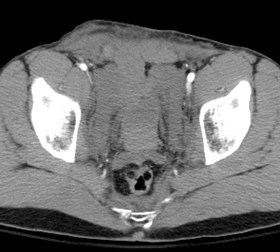
CT cystogram in patient with pelvic fractures


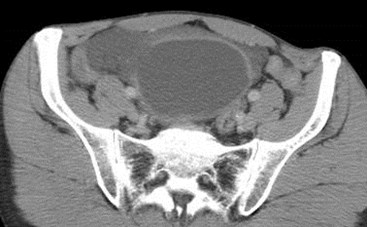

Extra Peritoneal Bladder Tear
Initial CT
CT Cystogram
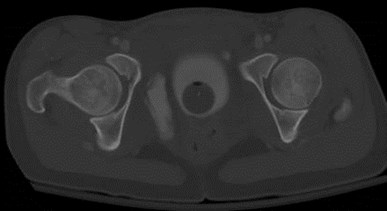

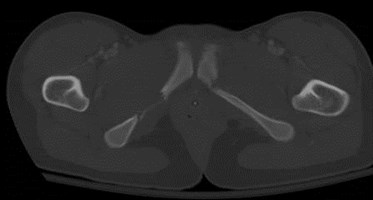
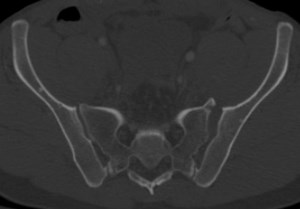
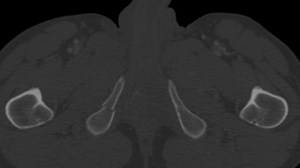
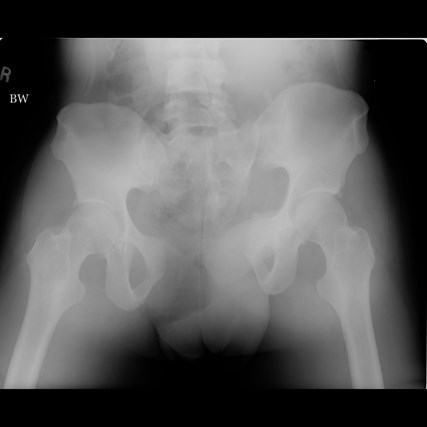
Pelvic Fractures
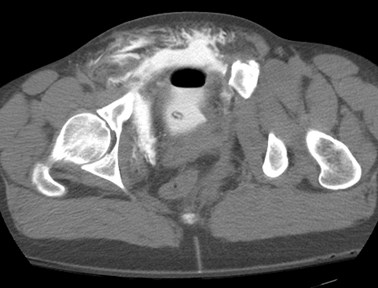
CT Cystogram: Extraperiteonal Bladder Tear
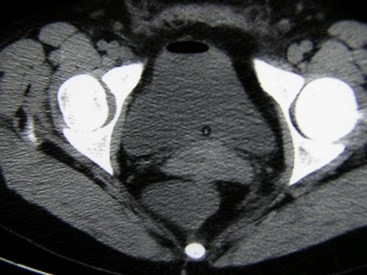
CT Cystogram: Intraperitoneal Bladder Tear


CT with liver and bowel injuries went to OR



Intraperitoneal Bladder Tear
Post operative imaging

Intra and extra peritoneal bladder rupture
Normal male urethral anatomy in the sagittal plane.
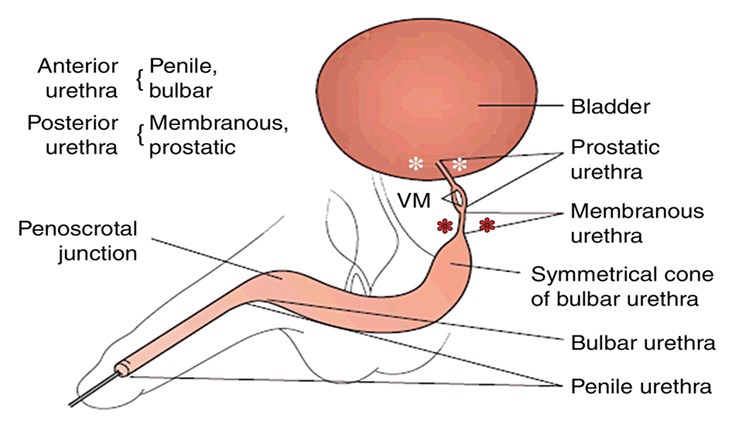
Ingram M D et al. Radiographics 2008;28:1631-1643


Pelvic Fractures
Retrograde Urethrogram
Grade 3 urethral injury: involves bulbar-membranous urethra

Initial CT

Pelvic fractures, molar tooth hematoma, bladder elevated out of pelvis



Foley placed with difficulty, had post op cystogram
Bladder neck injury: Type 4

Injury to posterior urethra
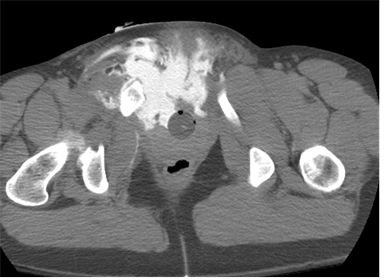
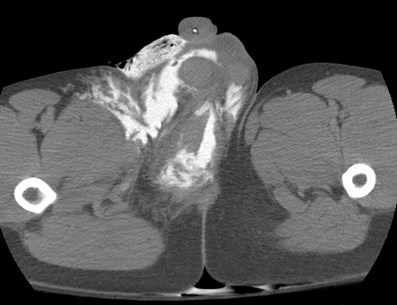
Combination urethral injury and
extra peritoneal bladder tear with
extravasation throughoutperineum, soft tissues, thigh andskin
Urethral Injuries
Majority occur in posterior urethra
–MVC, falls
–Bladder injuries in 20%
Approximately 1/3 anterior urethra
–Usually related to straddle injuries
Very rare in female urethra
Suspicious signs: blood at meatus, inability tovoid, pelvic/perineal hematoma

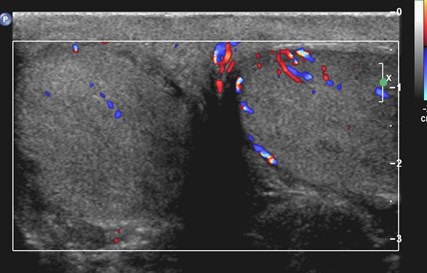
Testicular Contusions
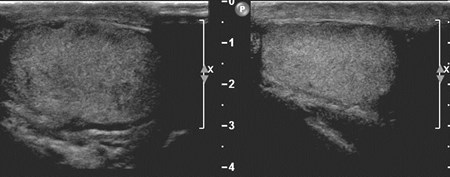


Testicular Contusion
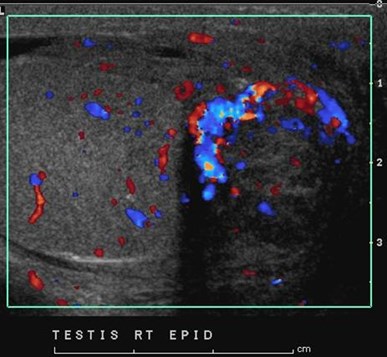
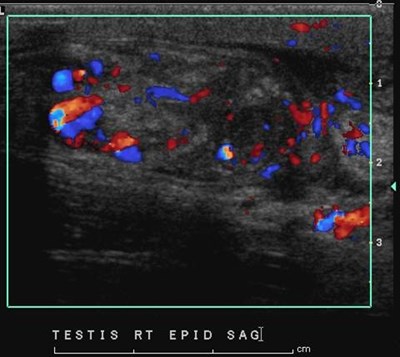
Epididymis injury with “traumatic”epididymitis

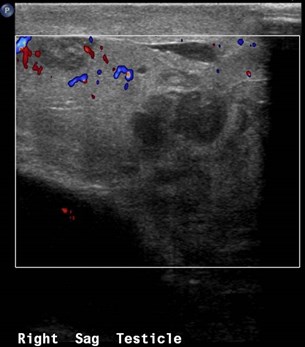
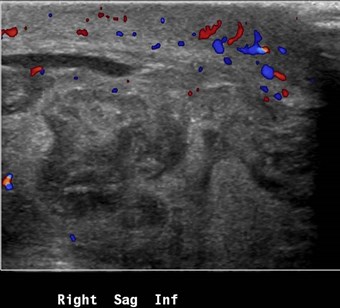
Intratesticular hematoma with rupture
Outcomes
Advances in staging techniques resulting from theincreased use of CT, increasing availability ofminimally invasive techniques such as angiographicembolization, and improvement of intensive care unitfacilities have resulted in increasing trend towardexpectant management
Surgical intervention now performed in only 5%–10%of renal injuries and continues to decline in frequencyof use
The End