
Tubes and LinesWhat, Where andWhoops
Tubes and LinesWhat, Where andWhoops
© William Herring, MD, FACR
All photos retain the rights of their original owners
Format of Lecture
For each device
What they are and what they do
Where they belong
Whoops – malpositioning andcomplications
Tube or Line
Desired Position
ETT
Tip > 5cm from carina
Tracheostomy tube tip
½way between stoma and carina
Central venous catheter
Tip in SVC
PICC Line
Tip in SVC
Swann-Ganz Catheter
Tip in proximal R or L Pulmonary Artery
Pleural Drainage Tube
Anterosuperior for PTX;posteroinferior for effusion
Pacemaker
Tip at apex of R ventricle; other(s) in RAand/or coronary sinus
AICD
One lead in SVC; other in R ventricle
NG tube
Tip in stomach
Airways
Endotracheal TubesWhat They Are Used For
Endotracheal TubesWhat They Are Used For
Indications for
Assisted ventilation
Isolate trachea to permit control of airway
Prevents gastric distension
Direct route for suctioning
Administration of medications via ETT
Endotracheal TubesWhere
Endotracheal TubesWhere
Tip should be at least 5cm above carina
Between clavicles and carina
Carina usually at level of T4
Tip may change by 2cm with flexion/extension
Balloon should never distend trachealwalls; if >2.8 cm, suspect laceration
Endotracheal TubesWhoops
Endotracheal TubesWhoops
Most common malposition: tip in rightmainstem bronchus
Leads to atelectasis, or
Right-sided tension pneumothorax
Tube in larynx or pharynx
Damage vocal chords
Aspiration
Chronic: Sinusitus 2° nasal mucosa edema
R3
Tip of endotracheal tube (yellow arrow) lies well above the carina (green arrow)
TracheostomyWhat
Indications for
Airway obstruction at or above level of larynx
Respiratory failure requiring long-termintubation (>21 days)
Obstruction during sleep apnea
Paralysis of muscles that affect swallowing orrespiration
TracheostomyWhere
TracheostomyWhere
Tip half-way between stoma and carina
About T3
Tip placement not affected by flexion/extension
Width of tube about 2/3 width of trachea
TracheostomyWhoops
TracheostomyWhoops
Immediately after
Subcutaneous emphysema
Pneumomediastinum
Pneumothorax
Cuff should not be >1½ times diameter oflumen
Tracheal stenosis
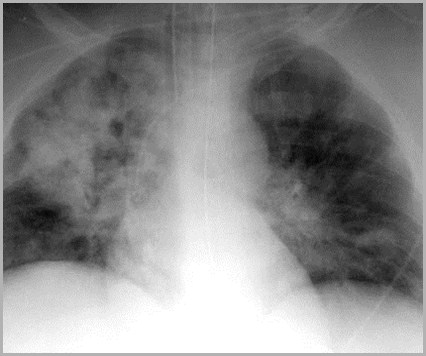
TracheostomyTracheal Stenosis
TracheostomyTracheal Stenosis
Most common late-occurring complication oftracheostomy tube
May occur at stoma, level of cuff or at tip oftube
Most common at stoma
Fibrosis with destruction of cartilage
At cuff site, usually 2° to circumferential scar
R3
Tip of tracheostomy tube (yellow arrow) lies about midwaybetween the stoma (blue arrow) and carina (green arrow)
Intravascular Lines
Central Venous CathetersWhat
Used in critically ill patients
For venous access
Measurement of central venous pressure
Intravascular blood volume
Central Venous CathetersWhere
Subclavian joins brachiocephalic veinbehind medial end of clavicle
Catheter should reach this point beforedescending
Catheter should descend lateral tospine and tip should be in the SVC
Central Venous CathetersWhoops
Most often malpositioned in RA orinternal jugular
Arrythmias in RA; inaccurate CVP readingselsewhere
Occasionally outside blood vessel
Look for sharp bends in catheter
Arterial placement suggested bypulsatile flow
Central Venous CathetersComplications
Air embolism
Pneumothorax (5%)
Hemothorax
Cardiac perforation
Sepsis
Venous perforation
Central Venous CathetersTwo or more attempts
Central Venous CathetersTwo or more attempts
Should initial placement fail, geta chest x-ray before trying otherside to avoid bilateralpneumothoraces
R3
Tip of central venous catheter (yellow arrow) curves gentlydownward into superior vena cava
PICC LinesPercutaneous Intravascular Central Catheters
PICC LinesPercutaneous Intravascular Central Catheters
What
Used for long-term access
Because of small size
Inserted through antecubital vein
Where
Tip should lie within SVC
Whoops
Tips may become malplaced over time
Pulmonary Artery CathetersWhat
Pulmonary Artery CathetersWhat
Swann-Ganz catheters
Aid in differentiating cardiac fromnon-cardiac pulmonary edema
Pulmonary Artery CathetersWhere
Pulmonary Artery CathetersWhere
Tip should lie within right or leftpulmonary artery
2cm from hila
Balloon inflated only whenmeasurements are made
Pulmonary Artery CathetersWhoops
Pulmonary Artery CathetersWhoops
Most common significant complicationis pulmonary infarction
From occlusion by catheter
From embolization off of catheter
Uncommon
Cardiac arrhythmia
Pulmonary artery perforation
Intracardiac knotting
R3
Tip of transabdominal Swan-Ganz catheter (yellow arrow)lies in right pulmonary artery
Pleural Drainage TubesWhat
Used to remove either air in or fluid inthe pleural space
Pleural Drainage TubesWhere
Pleural Drainage TubesWhere
Ideal position is anterosuperior for PTXand posteroinferior for effusion
Usually work well no matter wherepositioned
None of the side holes should lie outsideof the thoracic wall
Pleural Drainage TubesWhoops
Pleural Drainage TubesWhoops
Bleeding 2° laceration of intercostal artery
Laceration of liver or spleen on insertion
Insertion into the lung may lead to
Lung laceration
BP fistula
Rapid expansion of lung may lead topulmonary edema
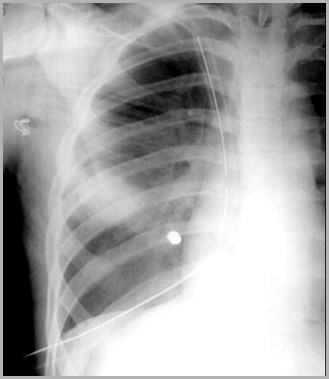
R3
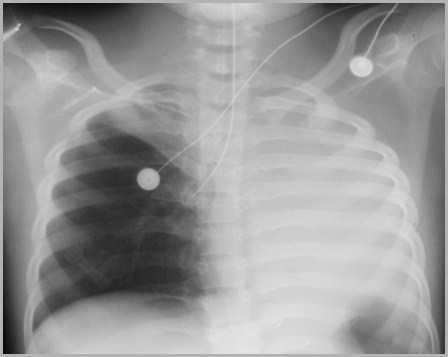
Tip of thoracostomy (pleural) drainage tube (yellow arrow) lies in the apexof the right hemithorax. The side hole (blue arrow) is well within the chest.
Cardiac Devices
Used for cardiac conductionabnormalities
Catheter should have gentle curves
PacemakersWhat
Tip positioned at apex of right ventricle
Tip may have slight bend as it abuts wall ofright ventricle
Not a sharp bend
Some pacers may also have lead(s) inright atrium and/or coronary sinus
PacemakersWhere
Fracture of leads at pacer, tip or site ofvenous access
Leads can perforate heart ➙ cardiactamponade
Look for sharp bends in leads 2° perforation ofblood vessel
Leads may be ectopically placed, e.g.hepatic vein
Pacemaker battery may migrate subcu
PacemakersWhoops

Two-lead pacemaker (red circle) shows one lead in right atrium (greenarrow) and the second in the right ventricle (red arrow).
Implantable DefibrillatorsWhat
Automatic implantable cardiac defibrillators(AICD)
AICDs used to prevent sudden death fromventricular defibrillation
Implantable DefibrillatorsWhere
Usually can be recognized by short,wider electrode on one or both leads
One electrode usually in SVC orbrachiocephalic vein
Other is in right ventricle
Implantable DefibrillatorsWhoops
Leads may fracture or migrate
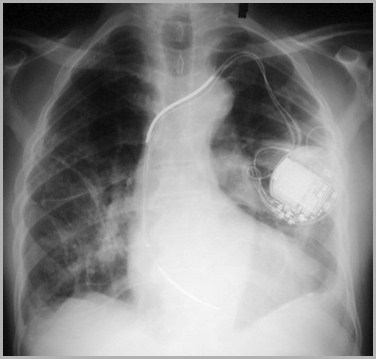
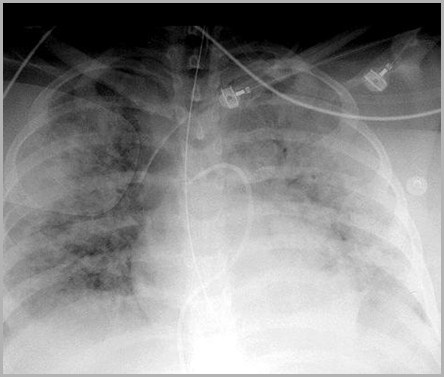
Two-lead automatic implantable cardiac defibrillator. You can differentiatethis from a pacemaker by the ‘fuzzy leads” (red arrows) on an AICD.
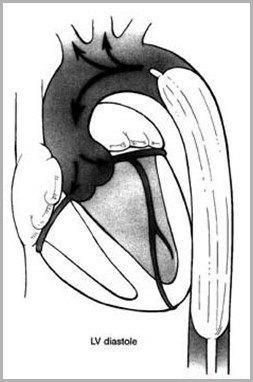
Intraaortic Balloon PumpWhat
Intraaortic counterpulsation balloon pump(IACB or IABP)
Used to improve cardiac output followingsurgery or in patients with cardiogenicshock
Inflated in diastole and deflated in systole
Increases O² to myocardium and decreases LVworkload
Intraaortic Balloon PumpWhere
Tip identified by small, rectangularmetallic marker
Should lie distal to left subclavian
Metallic marker should point slightly to right inregion of arch
www.CTSnet.org
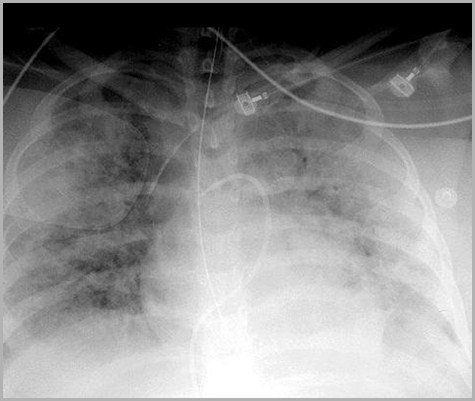
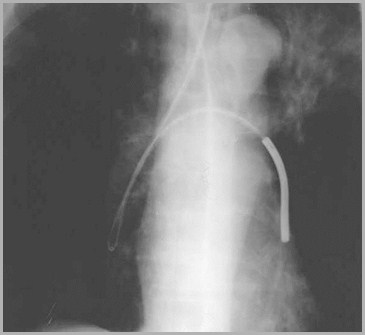
Tip of intra-aortic balloon pump (red arrow) lies just below top of theaortic arch (green arrow) and heads slightly to the right.
Intraaortic Balloon PumpWhoops
If catheter is too proximal, balloon mayocclude great vessels leads to stroke
If balloon is too distal, leads to decreasedeffectiveness
Aortic dissection may occur
Tip of intra-aortic balloon pump (yellow arrow) lies about2 cm from top of aortic arch (blue arrow)
R3
GI Tubes and Lines
Indications for a NGT
Feeding
Gastric sampling and decompression
Administering medication
Nasogastric TubesWhat
Tip should be in stomach
At least 10 cm of tube should extend intostomach
Many have side holes that extend up to 10cmon tube
Nasogastric TubesWhere
Most commonly malpositioned of all tubesand lines
May enter trachea and bronchi or curl inesophagus
Perforation usually involves cervicalesophagus
Can also perforate stomach
Indwelling tube leads to G-E reflux
May cause esophagitis and stricture
Nasogastric TubesWhoops
Tip of nasogastric tube (yellow arrow) should lieat least 10cm into the EG junction

Feeding TubesWhat, Where and Whoops
What
Used for nutrition
Where
Tip of feeding tube should be in duodenum
Most are in the stomach
Whoops
Perforation by guide wire
Too proximal ➙ aspiration
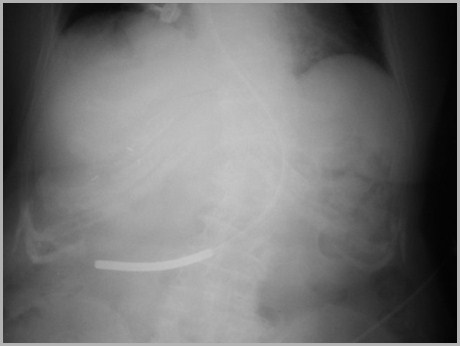
The tip of the feeding tube (green arrow) lies in theregion of the duodenal bulb. Ideally the tip should be in the duodenum.
Tubes and LinesThat HaveLost Their Way
See if you can tell what’s wrongwith the placement of these tubes and lines
R3
Feeding tube (green arrow) enters right lower lobe bronchus, loops onitself then crosses over to LLL bronchus (red arrow).

R3
Tip of central venous catheter coils back on itself in rightbrachiocephalic vein (red arrow).
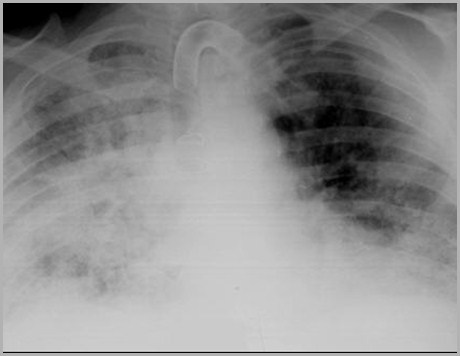
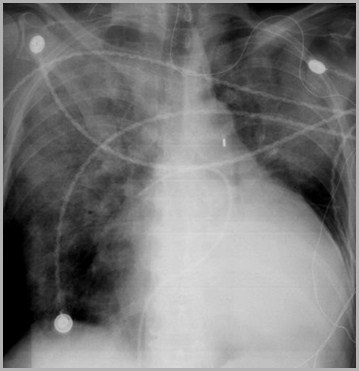
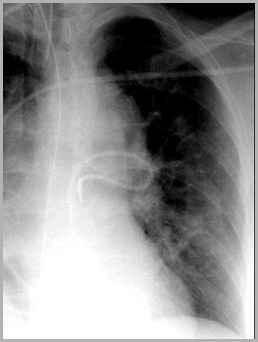
Tip of endotracheal tube is in right mainstem bronchus (redarrow) so right upper lobe and entire left lung are atelectaticbecause they are not being aerated.
R3
Swann-Ganz catheter enters left pulmonary artery (red arrow),then loops back on itself with tip in region of right ventricularoutflow tract (green arrow)
R3
Tip of Swan-Ganz catheter lies too peripherally in rightdescending pulmonary artery (red arrow)
R3
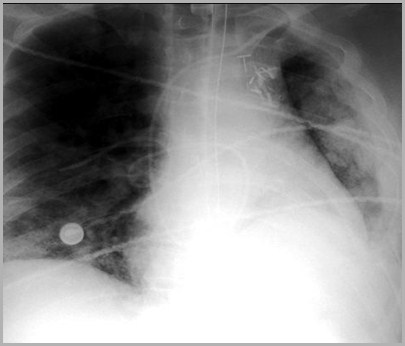
Tip of pleural drainage catheter (thoracotomy drainage tube) enterson right and crosses mid-line to the opposite side (red arrow).
