
Test YourselfOn the ABCsOf Heart Disease
© William Herring, MD, FACR
The next slide is a review of thescheme for evaluating the heart fromthe frontal chest x-ray
Review
A
Is the Left
Atrium
Enlarged?
If yes,
then
If no,
then
Look at the
Pulmonary
Vasculature
Normal
Increased
Pulmonary
venous
hypertension
B
Is the Main
Pulmonary
Artery Big
or
Bulbous?
If yes,
then
If no,
then
Look at the
Pulmonary
Vasculature
C
Is the Main
Pulmonary
Artery
Segment
Concave?
If yes,
then
If no,
then
D
Is the
Heart
Dilated or
Delta-
Shaped?
If yes,
then
Don't Look at
Pulmonary
Vasculature.
Look at Aorta
Normal
Increased
Pulmonary
hypertension
Cardiomyopathy
Pericardial
Effusion
Multiple valve dz
Mitralregurgitation
Mitral
Stenosis
L Myxoma
VSD, PDA
Pulmonic
stenosis
ASD
(VSD)
Idiopathic
2° to lung dz
Normal
Ascending
dilated
Whole Aorta
Dilated
Cardiomyopathy
Aortic
Stenosis
Aorticregurgitation
HBP

Unknowns
Unknowns
Unknown Case 1
Here is unknown 1.It’s a 43 year-old female with shortness of breath.
The first question to ask is : A - Is the left atriumenlarged? To answer that question, you look at thecardiac contour where you will see left atrialenlargement. Is there a concavity there or is it straightor convex outward?
If you said the left atrium is not enlarged, you werecorrect. There is a normal concavity where the yellowarrow is.
The next question to ask is: B – Is the main pulmonaryartery (MPA) big? To answer that question you need todraw the tangent line from the apex of the left ventricleto the aortic knob and determine if the MPA protrudesbeyond the tangent line.
If you said the MPA protrudes beyond the tangent line(yellow arrow), you were correct. This is a “B” heart.
B
Is the Main
Pulmonary
Artery Big
or
Bulbous?
If yes,
then
Look at the
Pulmonary
Vasculature
Normal
Increased
Pulmonary
hypertension
Pulmonic
stenosis
ASD
(VSD)
Idiopathic
2° to lung dz
This is the algorithm for a “B” heart. The next thing you needto look at is the pulmonary vasculature. You have threechoices for the pulmonary vasculature for a “B” heart:
• Normal flow
• Increased flow
• Pulmonary arterial hypertension
31
The next thing to look at is the right descendingpulmonary artery (RDPA). In normal people it usuallymeasures less than 17 mm. It has been measured foryou in this patient. It measures 31 mm.
31
That excludes “Normal vasculature” and leaves eitherIncreased flow to the lungs or pulmonary hypertension.Next look at the peripheral pulmonary vasculature.
If you think the peripheral pulmonary vasculature looksincreased, then this is increased flow to the lungs.
If you think the peripheral pulmonary vasculature looksnormal, then you have described a discrepancy in sizebetween the central vessels (which are enlarged) andthe peripheral vessels, which aren’t. That discrepancydefines pulmonary arterial hypertension.

Increased flowIncreased flow
To help you make that decision, hereis an inset of increased flow to thelungs.
The peripheral pulmonary vasculature is normalwhereas the central vasculature is prominent.
1 PulmonaryHypertension
1 PulmonaryHypertension
This is a case of pulmonary arterial hypertension, inthis instance primary or idiopathic pulmonary arterialhypertension.
Unknown Case 2

Here is unknown 2.It’s a 67 year-old female with hemoptysis.
The first question to ask is : A - Is the leftatrium enlarged? To answer that question,you look at the cardiac contour where youmight see left atrial enlargement. Is there aconcavity there or is it straight or convexoutward?
If you said the left atrium is enlarged, youwere correct. There is a bump outwardwhere a normal concavity should be.This is an “A” heart.
A
Is the Left
Atrium
Enlarged?
If yes,
then
Look at the
Pulmonary
Vasculature
Normal
Increased
Pulmonary
venous
hypertension
Mitralregurgitation
Mitral
Stenosis
L Myxoma
VSD, PDA
PulmonaryArterialHypertension
Mitral
Stenosis
VSD,PDA
This is the algorithm for an “A” heart. The next thing youneed to look at is the pulmonary vasculature. You have fourchoices for the pulmonary vasculature for an “A” heart:
• Normal flow
• Pulmonary venous hypertension
• Increased flow
• Pulmonary arterial hypertension
19
The next thing to look at is the rightdescending pulmonary artery (RDPA). Innormal people it usually measures lessthan 17 mm. It has been measured for youin this patient. It measures 19 mm.
Next look at the peripheral pulmonaryvasculature. We’re going to compare thesize of the vessels at the base with those atthe apex. The next slide has blown upinsets of the apex and base.

Compare the size, not thenumber, of the vessels atthe apex and base.Normally the vessels atthe base should be largerthan those at the apexwith the person in theerect position. Is that truehere?
In this person, thevessels at the apex arelarger than those at thebase. This iscephalization. What kindof pulmonary vasculaturedoes cephalizationimply?
If you said pulmonary venous hypertension(PVH), you were correct. What is the firstdiagnosis in the “A” heart algorithm forpulmonary venous hypertension?
MitralStenosis
MitralStenosis
This is a patient with mitral stenosis.
Unknown Case 3

Here is unknown 3.It’s a 2 year-old male with a murmur.
The first question to ask is : A - Is the left atriumenlarged? To answer that question, you look atthe cardiac contour where you will see left atrialenlargement. Is there a concavity there or is itstraight or convex outward?
If you said the left atrium is not enlarged, youwere correct. There is a normal concavity wherethe yellow arrow is.
The next question to ask is: B – Is the mainpulmonary artery (MPA) big? To answer thatquestion you need to draw the tangent line fromthe apex of the left ventricle to the aortic knoband determine if the MPA protrudes beyond thetangent line. Does it?
If you said the MPA protrudes beyond the tangentline (yellow arrow), you were correct.This is a “B” heart.
B
Is the Main
Pulmonary
Artery Big
or
Bulbous?
If yes,
then
Look at the
Pulmonary
Vasculature
Normal
Increased
Pulmonary
hypertension
Pulmonic
stenosis
ASD
(VSD)
Idiopathic
2° to lung dz
This is the algorithm for a “B” heart. The next thing you needto look at is the pulmonary vasculature. You have threechoices for the pulmonary vasculature for a “B” heart:
• Normal flow
• Increased flow
• Pulmonary arterial hypertension
26
The first thing to look at is the right descendingpulmonary artery (RDPA). In normal people itusually measures less than 17 mm. It has beenmeasured for you in this patient at 26 mm.
26
That excludes “Normal vasculature” and leaveseither Increased flow to the lungs or pulmonaryhypertension. Next look at the peripheralpulmonary vasculature.
26
If you think the peripheral pulmonary vasculaturelooks increased, then this is increased flow to thelungs.
26
If you think the peripheral pulmonary vasculaturelooks normal, then you have described adiscrepancy in size between the central vesselsand the peripheral vessels.

PAH
To help you make that decision, hereis an inset of PAH.
If you said increased flow to the lungs, you werecorrect. Look at the algorithm for a “B” heart underincreased flow. What are the diseases listed?
This patient had an atrial septal defect.
AtrialSeptalDefect
AtrialSeptalDefect
Unknown Case 4

Here is unknown 4.It’s a 57 year-old male with chest pain.
This is obviously a “D” heart. If youfollowed the ABCs schema in a systematicfashion, you would come to the sameconclusion.
This is the algorithm for a “D” heart. There are two major causes of a dilated or a delta-shaped heart:
• Cardiomyopathy
• Pericardial effusion
D
Is the
Heart
Dilated or
Delta-
Shaped?
If yes,
then
Cardiomyopathy
Pericardial
Effusion
Multiple valve dz
It is oftenimpossible todifferentiate apericardialeffusion from acardiomyopathyfrom the chest x-ray alone. In thiscase, the heart isa typical “waterbottle” shape ofa pericardialeffusion. It hascontour-lessborders typicalof a largeeffusion.
Causes
• Viral
• TB
• Lupus
• Mets
• Trauma
• Post-MI
• Uremia
There arenumerouscauses for apericardialeffusionand it isusuallyimpossibleto find otherclues on thechest film totell you theexactcause. Howmanycauses canyou name?
The patient had uremic pericarditis.
Unknown Case 5(Last case)

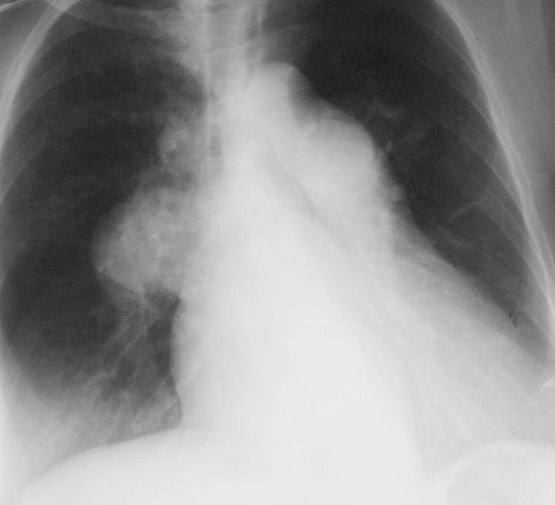
Here is unknown 5.It’s a 43 year-old male with syncope.
If you said the left atrium is not enlarged, youwere correct. There is a normal concavitywhere the yellow arrow is.
The next question to ask is: B – Is the mainpulmonary artery (MPA) big? To answer thatquestion you need to draw the tangent line fromthe apex of the left ventricle to the aortic knoband determine if the MPA protrudes beyond thetangent line. Does it?The next question to ask is: B – Is the mainpulmonary artery (MPA) big? To answer thatquestion you need to draw the tangent line fromthe apex of the left ventricle to the aortic knoband determine if the MPA protrudes beyond thetangent line. Does it?
The next question to ask is: C - Is the MPAsegment concave? Is it more than 15mm fromthe tangent line?
17
The answer to question C is yes.This is a “C” heart.
17
This is the algorithm for a “C” heart. Since almost all “C”hearts have normal pulmonary vasculature, that won’t helpto differentiate one from another. So we will look at theconfiguration of the thoracic aorta. In particular:
Is the thoracic aorta entirely normal?
Is only the ascending aorta prominent?
Is the entire thoracic aorta abnormal?
C
Is the Main
Pulmonary
Artery
Segment
Concave?
If yes,
then
Don't Look at
Pulmonary
Vasculature.
Look at Aorta
Normal
Ascending
dilated
Whole Aorta
Dilated
Cardiomyopathy
Aortic
Stenosis
Aorticregurgitation
HBP
Configuration of the Aorta
The next slide reviews the segmentsof thoracic aorta that can be abnormal
What you are trying to decide with a“C” heart is:
Is the thoracic aorta entirely normal
Is only the ascending aorta prominent
Is the entire thoracic aorta abnormal

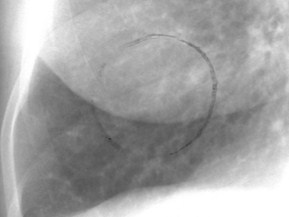
Aorticknobmeasures< 35mm
Descendingaortaswings farto left ofspine
Ascendingaortaprotrudesbeyondright heartborder
AbnormalAortic
Contours
AbnormalAortic
Contours
What do you think about the aorta in our case?Is it entirely normal, is only the ascendingaorta prominent or is the entire thoracic aortaabnormal?
What do you think about the aorta in our case?Is it entirely normal, is only the ascendingaorta prominent or is the entire thoracic aortaabnormal?
If you said only the ascending aorta isabnormally prominent, you were correct.What’s the diagnosis?
If you said only the ascending aorta isabnormally prominent, you were correct.What’s the diagnosis?
Aortic
Stenosis
Aortic
Stenosis
The End
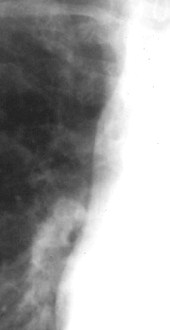
Normal
Only the ascending aorta is abnormallyprominent. See inset at left for the normalappearance of the ascending aorta.