
Cyanotic HeartDisease
Cyanotic HeartDisease
© William Herring, MD, FACR
Cyanosis With Increased Vascularity
Tricuspid atresia*
Transposition*
Truncus types I, II, III
TAPVR
Single ventricle
* Also appears on DDx of Cyanosis with Vascularity
Cyanosis With Decreased Vascularity
Tricuspid atresia*
Transposition*
Tetralogy
Truncus-type IV
Ebstein's
* Also appears on DDx of Cyanosis with Vascularity
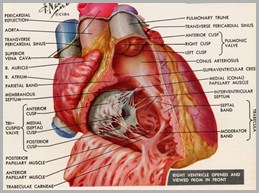
Tetralogy of Fallot
Tetralogy of Fallot
About 10% of all congenital heart lesions
Most common cause of cyanotic heartdisease beyond neonatal period
Tetralogy of FallotGeneral
Tetralogy of FallotComponents
High VSD
Pulmonic stenosis, i.e. rightventricular outflow obstruction
Usually infundibular, sometimesvalvular
Overriding of the aorta
Right ventricular hypertrophy

Tetralogy of FallotComponents
High VSD
Pulmonic stenosis, i.e. rightventricular outflow obstruction
Usually infundibular, sometimesvalvular
Overriding of the aorta
Right ventricular hypertrophy
Tetralogy of FallotOther Anomalies
Right aortic arch in 25%
Mirror image type
Left superior vena cava
ASD
Tricuspid valve abnormalities
Anomalies of coronary arteries
Aberrant left anterior descendingcoronary artery arising from rightcoronary artery
Tetralogy of FallotCritical Component
Degree of pulmonic stenosis
Regulates degree of R L shunt
Regulates overriding of aorta
Greater the stenosis, the greater theaortic overriding
Remember
Whenever there is a right-to-left shunt,there will be (some degree) of cyanosis
Tetralogy of FallotClinical findings
Squatting
Dyspnea
Failure to thrive
Cyanosis-usually
Severe cases at birth severe PS
Mild cases much later mild PS
“Pink tets” (acyanotic) and “Bluetets” (cyanotic)

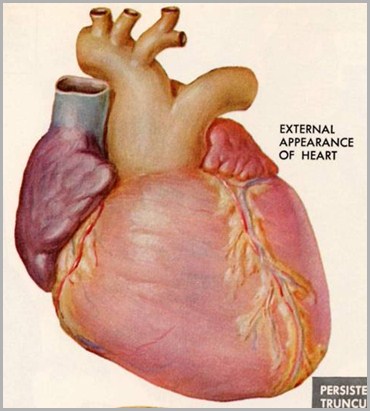
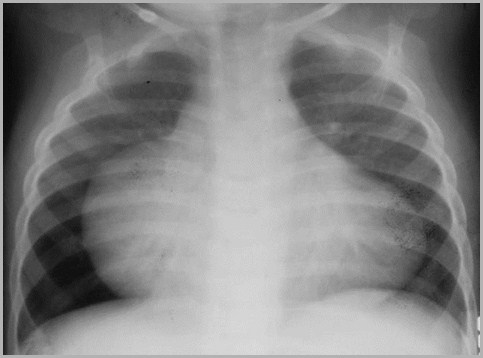
Tetralogy of FallotImaging Findings
Heart size normal
Rarely enlarged
Cardiac apex displaced upward “coeren sabot”
MPA segment concave
Decreased vasculature
Right aortic arch in 25%
Heart size normal
Cardiac apex elevated
Pulmonary arterysegment concave
DecreasedVasculature
R Ao Arch
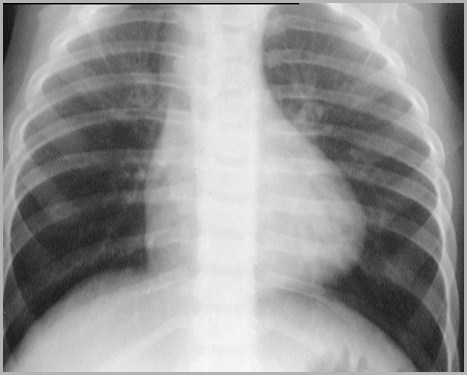
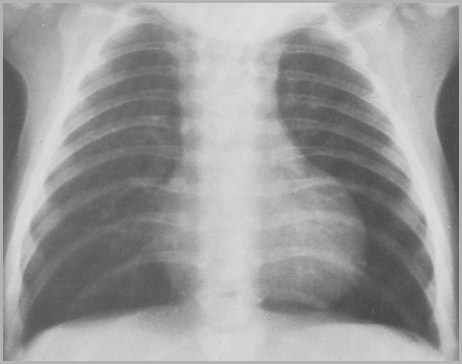
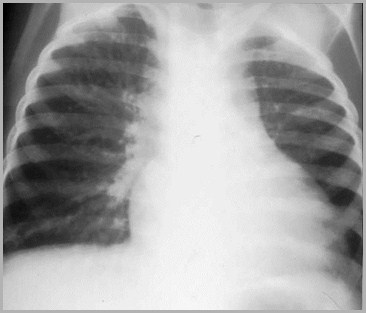
2 yo with Tetralogy of Fallot
2 yo with Tetralogy of Fallot
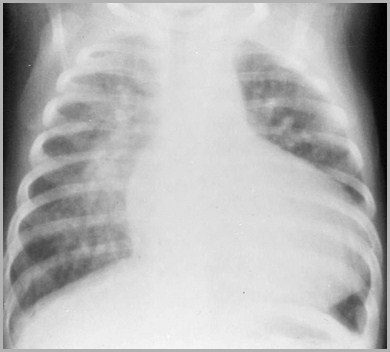
Heart size normal
Cardiac apex elevated
Pulmonary arterysegment concave
DecreasedVasculature
R Ao Arch
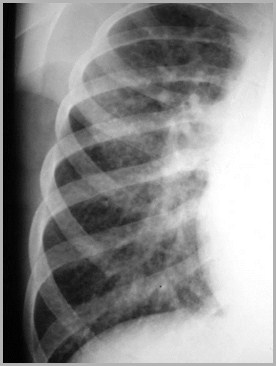
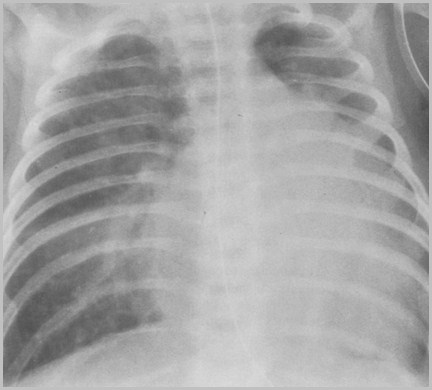
5 mos old with Tetralogy of Fallot

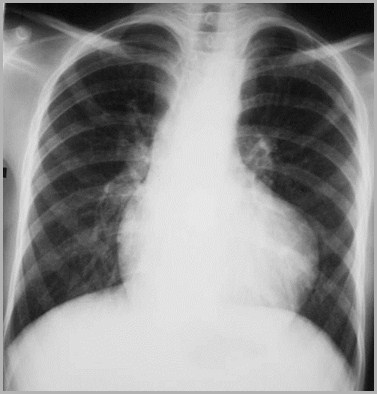
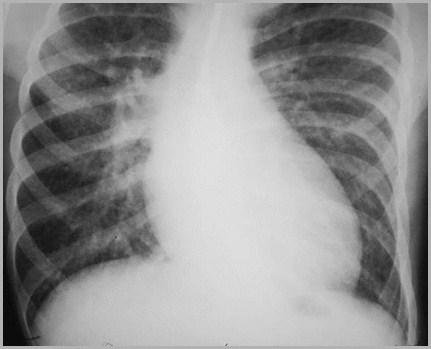
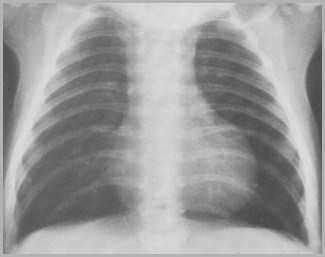
32 yo with Tetralogy of Fallot
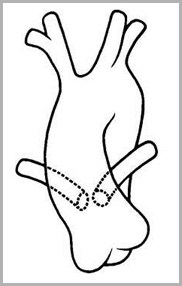
Tetralogy of Fallot
Overridingaorta
HighVSD
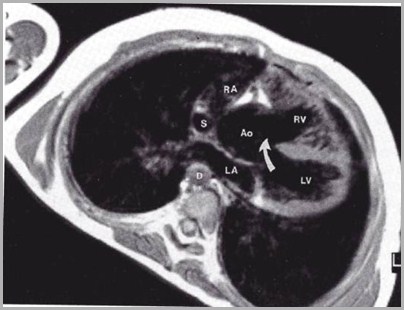
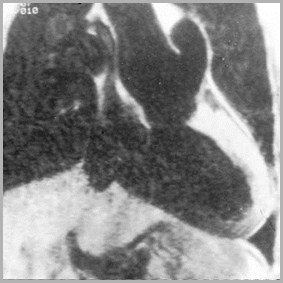
Tetralogy of Fallot

Axial spin-echo MRimage shows severeinfundibular stenosis(arrow).
Korean Journal of Radiology


Trilogy of Fallot
Pulmonic valvular stenosis
ASD
Right ventricular hypertrophy
TruncusArteriosus
TruncusArteriosus
Truncus ArteriosusEmbryology
Uncommon anomaly 2° failure ofprimitive common truncus arteriosus todivide into aorta and pulmonary artery

Truncus ArteriosusGeneral
The truncal valve is usually tricuspid
Main pulmonary artery segment isconcave in types II, III, and IV
Pulmonary vasculature is shunt type intypes I, II and III
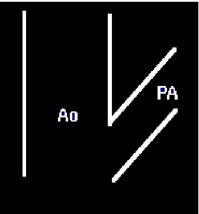
Commontrunk
Ao
PA
Truncus ArteriosusRight sided aortic arch
Right-sided arch in about 33%
Usually mirror-image type
But because truncus is so rare, itaccounts for only 6% of all right arches
Right aortic arch
Truncus ArteriosusTriad
Increased flow
Cyanosis
Cyanosis with Vascularity
Tricuspid atresia*
Transposition*
Truncus types I, II, III
TAPVR
Single ventricle
Truncus ArteriosusAssociations
VSD
Always
Anomalies of the coronary arteries
Truncus ArteriosusClinical Findings
Infants may demonstrate L R shunt
Minimal cyanosis
CHF
Respiratory infections
Growth disturbances
Majority are dead by 6 mos
Cyanosis is worse in II and III
Can’t tell them apart clinically
Associated anomalies
Bony
Renal
Lung
Cleft palate
Truncus ArteriosusClinical Findings
Truncus ArteriosusX-ray Findings
Cardiomegaly
Right aortic arch (33%)
Concave or convex-appearing MPA
Enlarged left atrium in 50%
Displacement of hilum
Elevated right hilum in 20%
Left hilum in 10%
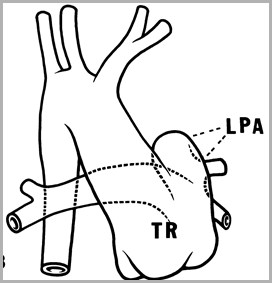
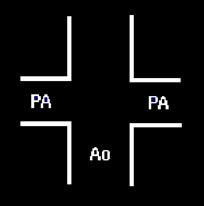
Truncus-Type I
Convex“pulmonaryartery”segment
Shuntvessels
PA arises onleft via shortcommon stem
Most common (75%)
Ao
Remember
Whenever blood is pumped intopulmonary circulation at or nearsystemic pressures, pulmonaryarterial hypertension will develop
LPA
Truncus
Ao
Ao
Truncus Type 1
LV
Truncus-Type II
Shunt vessels
Concave mainpulmonaryartery
Pulmonaryarteries ariseposteriorlyfrom aorta
Less common (25%)
Truncus Type II
Enlarged heart
Concave PAsegment
ShuntVessels
Truncus Type II
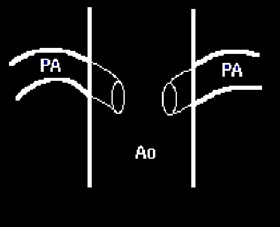
Truncus-Type III
Shunt vessels
Concave mainpulmonaryartery
Right and leftpulmonaryarteries ariselaterally
Rare (5%)

Truncus-Type IV
Concave mainpulmonaryartery
Bronchialcirculation
No pulmonaryarteries
Rare to non-existent
TOF withpulmonaryatresia
Truncus-Type IV(TOF with pulmonary atresia)
Bronchial Circulation

Increased flow
I
III
II
IV
Pulmonary artery
Shunt vessels
I
Convex
Yes
II
Concave
Yes
III
Concave
Yes
IV
Concave
Bronchialcirculation
Truncus Arteriosus
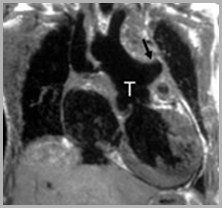
Single large artery (T) arising from heart
PA (arrow) originates from left side oftruncus
Amersham
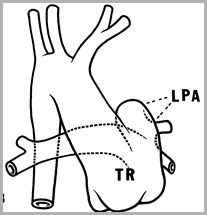
Truncus Arteriosus Type 1
TricuspidAtresia
TricuspidAtresia
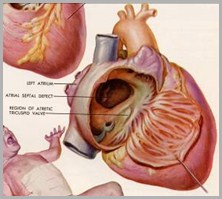
Tricuspid Atresia
Fusion of dorsal and ventral endocardialcushions occurs too far to the right obliteration of tricuspid valve, and
Hypoplasia of right heart
Tricuspid valve, right ventricle andpulmonary artery

Tricuspid AtresiaShunts needed
Complete obstruction to outflow from RA
Need R L shunt: Patent foramen ovale or ASD
Small ASD elevated RA pressures enlarged RA
Large ASD lower RA pressures minimalenlargement of RA
Blood in left heart must get back to lungs
Also have associated VSD or PDA
Tricuspid AtresiaTransposition of Great Vessels
70% have normal relationships of greatvessels
30% have transposition of great arteries
Tricuspid AtresiaTwo main types
No Transposition of the Great Vessels
Usually have PS
Majority (70%)
With Transposition of the Great Vessels
Usually no pulmonic stenosis
Minority (30%)
Tricuspid atresia—no transposition
(majority-some PS)
Tricuspid atresia—no transposition (70%)With some PS
Need R L shuntthrough patentforamen ovale
Someunsaturatedblood exitsaorta=cyanosis
Systemicblood cannot enterRV
Bloodenterslungs eitherthroughVSD or PDA
PA
Ao
Ao
PA
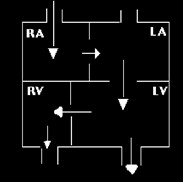
Tricuspid atresia—with transposition (30%)-No PS
Systemicblood cannot enterRV
Need R L shuntthrough patentforamen ovale
Un-oxygenatedblood flowsto lung viatransposedPA flow
Oxygenatedbloodreturns toLA
Need L Rshunt to getblood intobody
Tricuspid atresiaX-ray Findings - No transposition
Normal-sized heart
Decreased pulmonary vessels (60-70%)
Pulmonic stenosis usually present
Flat/concave pulmonary artery
Small ASD enlarged RA
Blood can’t exit RA
Large ASD normal or slightly RA
Blood can exit RA
Tricuspid atresia—some PS, no transposition
Normal-sizeheart
Decreasedpulmonaryvasculature
Concave MPA
RA notenlarged=largerASD
Tricuspid atresia—some PS, no transposition
Tricuspid atresiaX-ray Findings - Transposition
Mild cardiomegaly
Engorged pulmonaryvessels
No pulmonic stenosis
No characteristicappearance to heart
Ao
PA
Tricuspid atresia—no PS, shunt vessels
Enlarged heart
Shunt vessels
Tricuspid atresia—no PS, shunt vessels
Why Tricuspid Atresia Appears on BothIncreased and Decreased Vasculature DDxswith Cyanosis

With PS
Without PS
Tricuspid atresia

ECG-gated spin-echotransaxial imagedemonstrates a bar ofmuscle and fat (bluearrow) (tricuspid atresia)separating the rightatrium (yellow arrow)from the hypoplasticright ventricle (redarrow)
Amersham
Tricuspid atresia
Enlargedright atrium
Small rightventricle
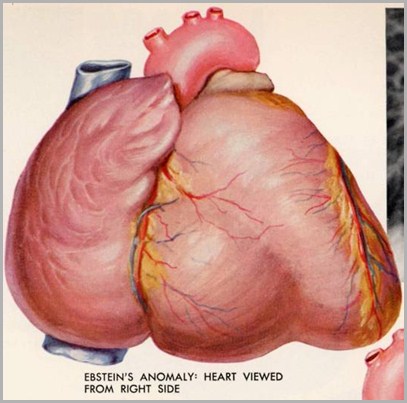
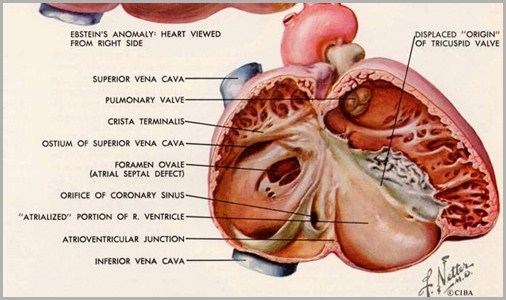
Ebstein’s Anomaly
Ebstein’s Anomaly
Ebstein’s AnomalyGeneral
Rare
Posterior and septal cusps of tricuspid valvedisplaced into right ventricle
Right ventricle smaller or “atrialized”
Tricuspid insufficiency right atrialpressure a R L shunt through foramenovale (or ASD)
Cyanosis is present in neonate
Ebstein’s Anomaly
Remember
Increased volume of blood from regurgitantvalves always produces larger sized chambersthan does blood under increased pressure asin a stenotic valve
Ebstein’s Anomaly
Normal
Ebstein’s AnomalyX-ray Findings
Cardiomegaly
One of only conditions cardiomegalyfirst few days of life
Unusual prominence to right heart border
Pulmonary flow is decreased

Ebstein’s
Anomaly
Ebstein’s
Anomaly
Markedcardiomegaly
Decreasedvasculature
Cyanosis
Ebstein’s
Anomaly
Ebstein’s
Anomaly
Ebstein’s Anomaly
Ebstein’s Anomaly
Ebstein’s AnomalyTriad
Decreased flow
Cyanosis
MarkedCardiomegaly
Cyanosis with Dec vascularity
Tricuspid atresia*-normal
Transposition*-normal
Tetralogy-normal
Truncus-type IV-enlarged
Ebstein's-huge
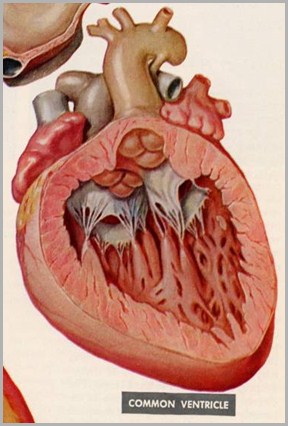
Single Ventricle
Single Ventricle
Single Ventricle
Surprise!
There are usually two ventricles in this disease
Single ventricle: one “normal” ventricle withtwo atria
Three types of Single Ventricle
Morphologic LV with a rudimentary RV (common)
Morphologic RV with a rudimentary LV (rare)
Morphologically indeterminate ventricle (rare)
Single Ventricle
Most common
Morphologic LV with rudimentary RV
Also called
Double-inlet left ventricle
Common ventricle
Univentricular heart
Frequently difficult to determinewhich anatomic ventricle is present
Single VentricleAssociated Findings
Pulmonic stenosis
Valvular or subvalvular (66%)
Pulmonary atresia
PAPVR
PDA
Single VentricleImaging Findings
No characteristic appearance
Concave pulmonary artery segment
Shunt vessels
Single ventricle
The End