
Diseases of theGreat VesselsDiseases of theGreat Vessels
All illustrations retain their original copyrights
© William Herring, MD, FACR
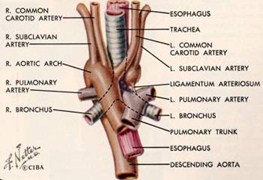
Aortic AnomaliesGeneral
Most are asymptomatic
Unless they causeencircling vascular ringlike pulmonary sling
Can be complexlesions requiringmultiple projections
MRI or CT
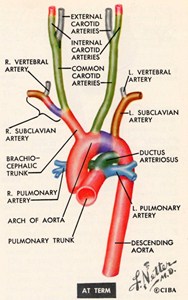
© Frank Netter, MD Novartis®
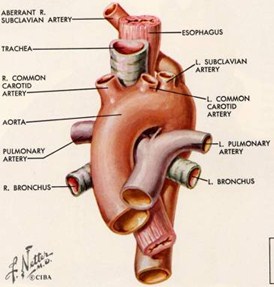
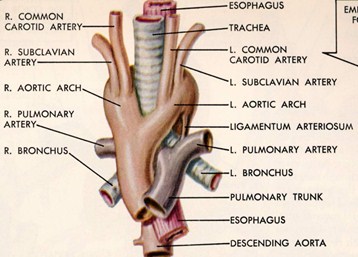
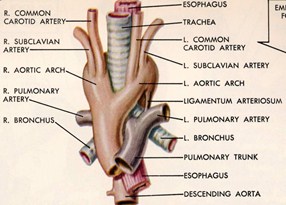
Aberrant Subclavian ArteriesGeneral
Left arch with aberrant right subclavian
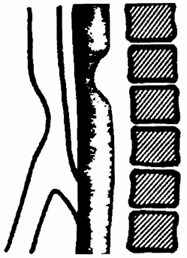
Usually passes posterior to esophagus
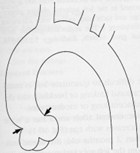
Dilated origin is “Diverticulum of Kommerell”
Right arch with aberrant left subclavian
Most are asymptomatic
Passes behind esophagus
Low incidence of congenital heart dz
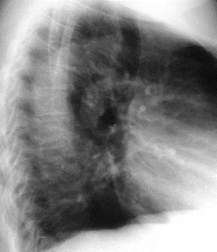
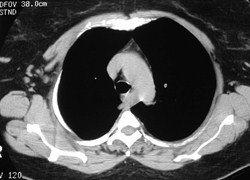
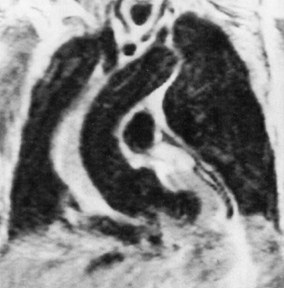
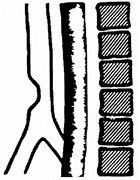
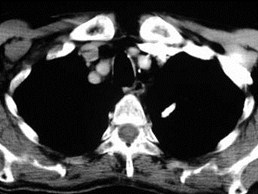
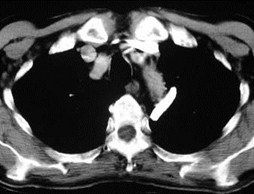
Left Aortic ArchWith Anomalous RSCA
Left Aortic ArchWith Anomalous RSCA
Left Arch with Anomalous RSCA
Occurs in less than 1% of people
Passes posterior to esophagus
Pushes trachea and esophagus forward
Produces oblique shadow aboveaortic arch on frontal film
Origin of RSCA may be dilated
Diverticulum of Kommerell
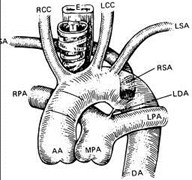
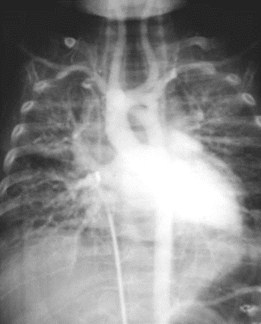
Left Aortic Arch with Aberrant R SCA
© Frank Netter, MD Novartis®
© Dahnert Lippincott Williams & Wilkins
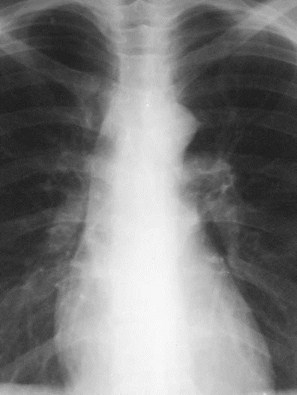
Left Aortic Arch with Aberrant Right SCA


Left Aortic Arch with Aberrant R SCA
© L. Elliott, MD J.B. Lippincott ®
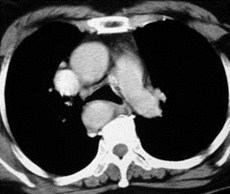
Right Aortic Arches
Right Aortic Arches
Right Aortic ArchTypes
At least five different types
Only two of importance
Right Aortic ArchTypes
Mirror Image Type — Type I
Aberrant left subclavian — Type II
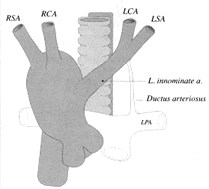
Mirror Image
Aberrant LSCA
© Stephen Miller, MD Mosby The Requisites
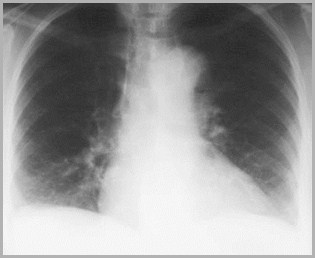
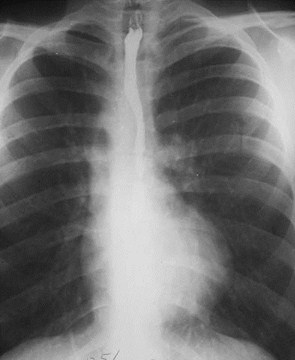
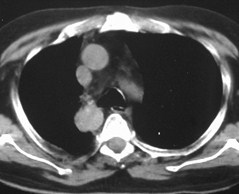
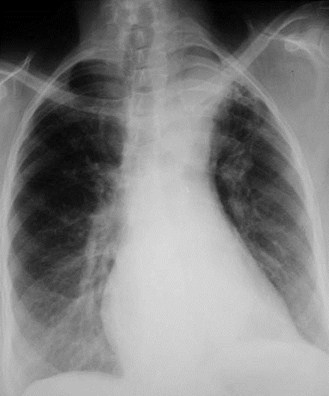
Right Aortic ArchesGeneral
Recognized by leftward displacement
Of barium-filled esophagus
Of air-filled trachea
Aortic knob is absent from left side
Aorta descends on right
Para-aortic stripe returns to left side ofspine just above diaphragm
Right Aortic ArchesGeneral
Mirror-image type almost always hasassociated CHD
Usually Tetralogy of Fallot
Aberrant Left Subclavian type rarelyhas associated CHD
Most common variety of right arch
Right Aortic ArchType 1—Mirror Image Type
2° interruption of left arch just distal toductus arteriosis
Associated with congenital heartdisease 98% of time
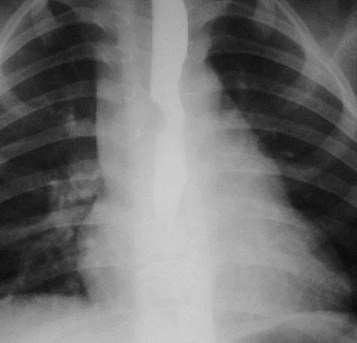
Right Aortic ArchType 1—Mirror Image Type–X-ray Findings
No posterior impression on trachea orbarium-filled esophagus
Heart is usually abnormal in size orshape
Aorta descends on right

Mirror Image Right Aortic Arch with TOF
Mirror Image Right Aortic Arch
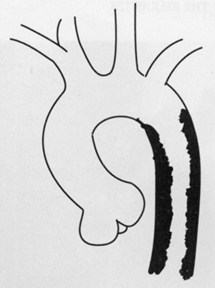
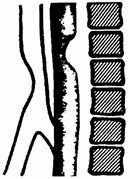
Right Aortic ArchType ll—Aberrant Left Subclavian
2° interruption of left aortic archbetween LCC and LSC arteries
Associated with cardiac defects 5-10%of the time
Tetralogy of Fallot most often (71%)
ASD or VSD next most often (21%)
Coarctation of aorta rarely (7%)
Right Aortic ArchType ll—Aberrant Left Subclavian
Anomalous left subclavian artery(retroesophageal and retrotracheal)
Aorta descends on right
© Frank Netter, MD Novartis®
Right Arch with Aberrant LSCA
© Stephen Miller, MD Mosby The Requisites
© Dahnert Lippincott Williams & Wilkins
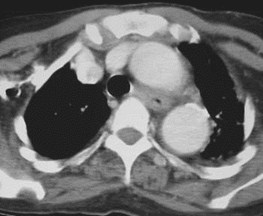
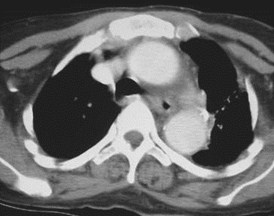
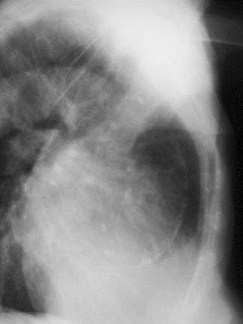
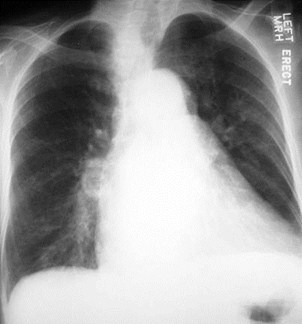
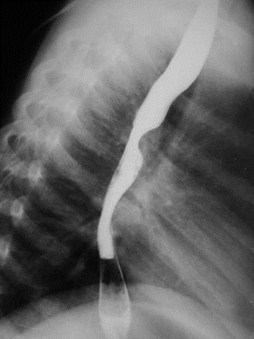
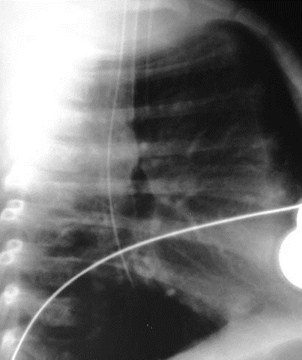
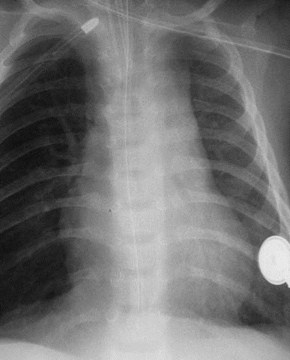
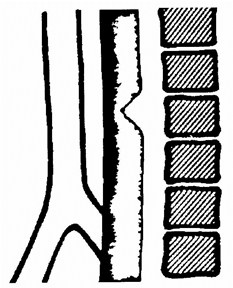
Right Aortic ArchAberrant Left Subclavian—X-ray Findings
Posterior impression on trachea andbarium-filled esophagus
Heart is usually normal in size andshape
Aorta descends on right
© Stephen Miller, MD Mosby The Requisites


Right Aortic Arch with Aberrant Left Subclavian
Right Aortic Arch with Aberrant Left Subclavian


Right Aortic Arch with Aberrant Left Subclavian
90% with Tetralogy of Fallot
6% with Truncus Arteriosis
5% with Tricuspid Atresia
If the patient hasa Mirror Right arch,
Then it will beassociated
Truncus arteriosis33%
Tetralogy of Fallot25%
Transposition10%
Tricuspid atresia5%
VSD2%
Apparent discrepancy due to muchhigher incidence of TOF than Truncus
If the patient hasthis disease,
This % will have aMirror Right arch
Right Aortic Arch withAberrant Left Subclavian
Mirror ImageRight Aortic Arch
Left Aortic Archwith Aberrant R SCA
A
B
C
Identify these three anomalies andtell whether they are usuallyassociated with congenital heartdisease or not
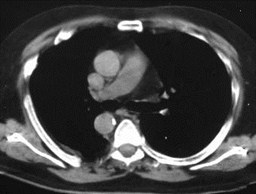
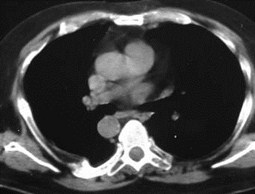
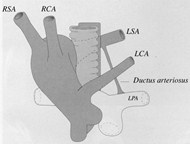
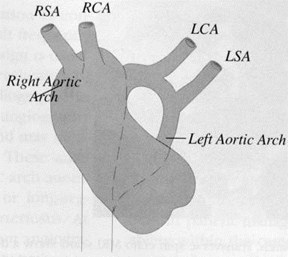
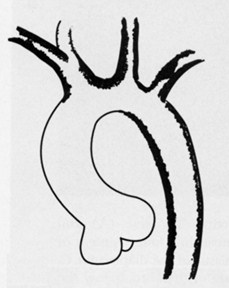
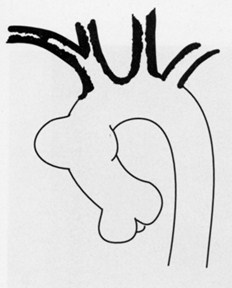
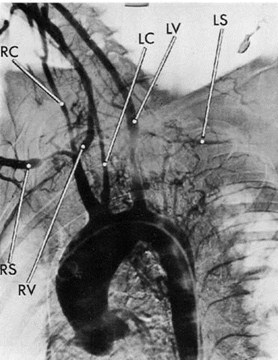
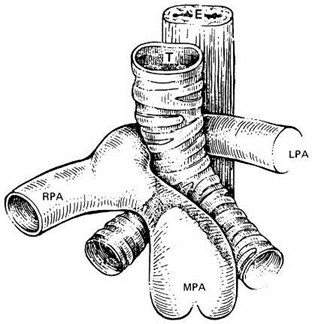
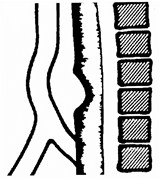
Double Aortic Arch
Double Aortic Arch
Double Aortic ArchGeneral
Most common vascular ring
Rarely associated with congenital heartdisease
But vascular ring tracheal and/oresophageal compression
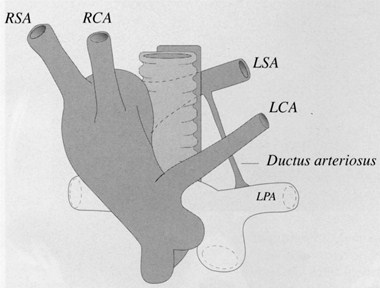
Caused by persistence of R and L IVbranchial arches
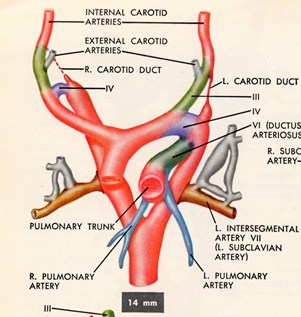
R IV arch normallybecomes mostproximal segmentof RSCA
L IV arch is part ofnormal aortic archbetween LCC andLSCA
Persistence of both IV branchial arches forms avascular ring or Double Aortic Arch
© Frank Netter, MD Novartis®
Passes on both sides of trachea
Joins posteriorly behind esophagus
Right arch is larger and higher
Left arch is smaller and lower
Ba swallow shows bilateral impressions onfrontal view
Posterior impression on lateral view
Angiogram is characteristic
Double Aortic ArchGeneral
Double Aortic ArchClinical
Symptoms may begin at birth
Symptoms include
Tracheal compression, or
Difficulty swallowing
Double Aortic ArchAnatomy
Right arch suppliesRSCA and RCC
Left arch suppliesLCC and LSCA
© Stephen Miller, MD Mosby The Requisites
Double Aortic Arch
© Frank Netter, MD Novartis®
© Dahnert Lippincott Williams & Wilkins
Double Aortic ArchX-ray Findings
Right arch is higher and larger
Left arch is lower and smaller
Produces reverse S on esophagram on AP
On lateral, arches are posterior toesophagus and anterior to trachea


Double Aortic Arch
Double Aortic Arch
© Frank Netter, MD Novartis®


Double Aortic ArchImpressions on Trachea and Esophagus
© Dahnert Lippincott Williams & Wilkins

Double Aortic Arch
Cervical AorticArch
Cervical AorticArch
Cervical Aortic ArchGeneral
Rare
Usually asymptomatic
May present as pulsating supraclavicularmass
May produce vascular ring and compressairway
Embryogenesis uncertain
Over 80% are right-sided
Cervical Aortic ArchImaging Findings–Right-sided lesions
Right-sided cervical aortic arches
Right apical mass-like density
Absence of aortic knob
Descend on the left
Displace the trachea and esophagus forward
Branching may be normal or mirror-image
Cervical Aortic ArchImaging Findings–Left-sided lesions
Left-sided cervical aortic arches
Aortic knob at apex of lung
Descend on the left
Do not displace the trachea or esophagusforward
Cervical Aortic Arch


Cervical Aortic Arch
Aortitis
Aortitis
Chronic inflammatory arteritis
Affects aorta, its main branches andpulmonary arteries
15-40 years, 8:1 females, Orientalpopulation
LSCA, LCCA, brachiocephalic, renals,celiac commonly involved
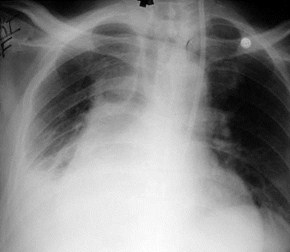
Takayasu’s Aortitis Pulseless Disease
Takayasu’s AortitisType 3
Most common isType 3 (55%)
Stenoses ofaortic arch,distal thoracicand abdominalaorta
© Stephen Miller, MD Mosby The Requisites
Takayasu’s AortitisType 2
Next mostcommon is Type 2(11%)
Segmentalstenoses indescendingthoracic andabdominal aorta
© Stephen Miller, MD Mosby The Requisites
Takayasu’s AortitisType 1
Next mostcommon is Type 1(8%)
Stenoses in arch,brachiocephalic,carotid andsubclavianarteries
© Stephen Miller, MD Mosby The Requisites
Takayasu’s Aortitis (Type 3)
© Stephen Miller, MD Mosby The Requisites
On angiography, narrowing of aorticlumen
On MRI, thickened aortic wall
Associated aneurysms may be saccularor fusiform
Takayasu’s AortitisImaging Findings
Other Forms of Aortitis
Inflammation of intima and media
Healing produces scarring - “tree-bark”appearance of luminal surface
Aorta dilates
Ascending aorta more than arch
Abdominal aorta spared
Opposite of atherosclerosis
Aortic wallbecomes thickenedon healing
Usually results inaortic regurgitation
Diastolic murmur
Other Forms of Aortitis
Giant Cell Arteritis
© Stephen Miller, MD Mosby The Requisites
Causes of Aortitis
Rheumatic fever
Reiter’s syndrome
Syphilis
Begins above sinotubular ridge
Giant cell arteritis
Ankylosing spondylitis
Crosses sinotubular ridge and dilates bothroot and ascending aorta
Sinotubular Ridge-Jct of Sinuses of Valsalvaand tubular aorta
© Stephen Miller, MD Mosby The Requisites
Syphilitic Aortitis
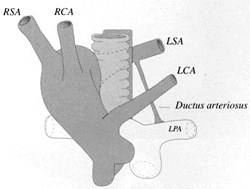
Pulmonary SlingPulmonary Sling
Pulmonary SlingEmbryogenesis
Failure of formation of left 6th aortic arch absence of left pulmonary artery
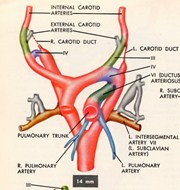
Proximal L VI archnormally becomesproximal segment of LPA; distal VI persistsas ductus until birth

© Frank Netter, MD Novartis®
Pulmonary SlingGeneral
Aberrant origin of left pulmonary artery
From the right pulmonary artery
Left pulmonary artery passes betweentrachea and esophagus
Most have other anomalies
Stenosis of right mainstem bronchus
May lead to air-trapping, lobar emphysema andhyperlucent lung
Pulmonary Sling
© Dahnert Lippincott Williams & Wilkins
© L. Elliott, MD J.B. Lippincott ®
Pulmonary SlingDDX
Only vascular malformation to passbetween esophagus and trachea
Bronchial cyst may produce samefinding on esophagus/trachea
Pulmonary Sling
Pulmonary Sling
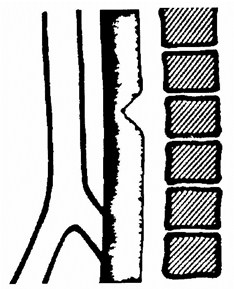
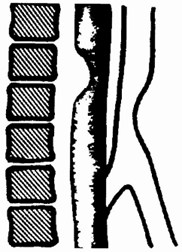
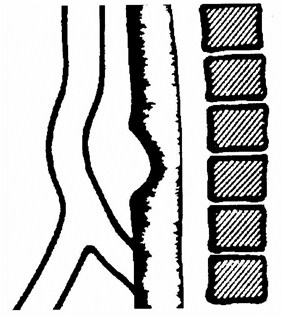
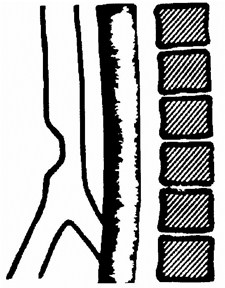
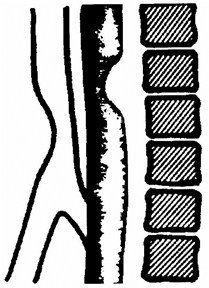
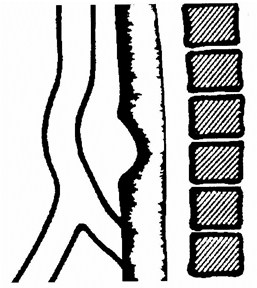
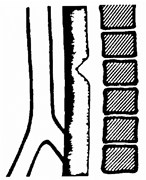
Tracheal Impressions
Posterior Esophagus
Anterior Trachea
Left Ao Arch with Aberrant R SCA
Right Ao Arch with Aberrant L SCA
Isolated anomalies
BCA arising too distal
CCA arising too proximal
CCA and BCA arising together
© Dahnert Lippincott Williams & Wilkins
© Dahnert Lippincott Williams & Wilkins
Anterior trachea andPosterior Esophagus
Posterior trachea andAnterior Esophagus
Double Aortic Arch
R Ao Arch with Aberrant LSCA + L ductus
L Ao Arch with Aberrant RSCA + R ductus
Pulmonary Sling
© Dahnert Lippincott Williams & Wilkins
© Dahnert Lippincott Williams & Wilkins
Aberrant SCA
Pulmonary Sling
Double Ao Arch
Isolated Anomalies
© Dahnert Lippincott Williams & Wilkins
Venous Anomalies
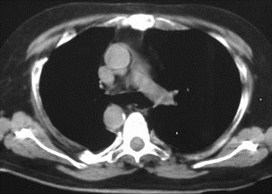
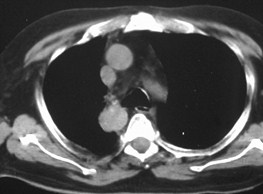
Venous Anomalies
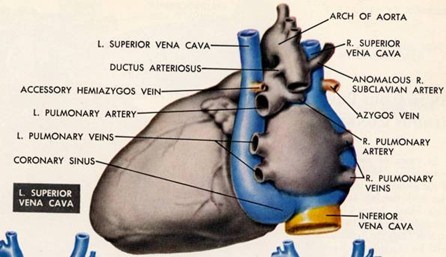
Persistent LeftSVC
Persistent LeftSVC
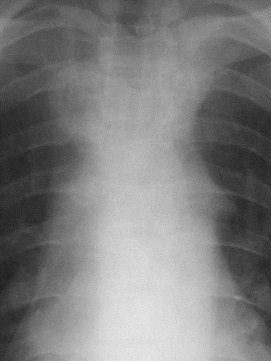
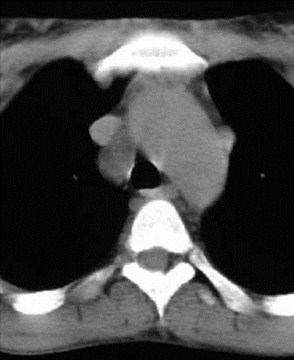
Persistent Left SVC
Occurs in less than 0.5% of people
Failure of regression of L common and Ant.Cardinal veins
Drains left jugular and left subclavian v
Most patients also have right-sided SVC
Drains into dilated coronary sinus Ratrium
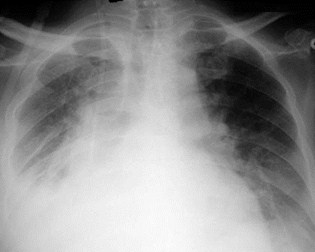
Post-op day 3
Post-op day 6




Persistent Left SVC


© Frank Netter, MD Novartis®
Diseases of theNot-So-GreatVessels
Diseases of theNot-So-GreatVessels
Left SuperiorIntercostal VeinAortic Nipple
Left SuperiorIntercostal VeinAortic Nipple
Left Superior Intercostal VeinThe Aortic Nipple
Visible in 5% of people
Should not be mistaken for mass
Aortic Nipple-Left SuperiorIntercostal Vein


Aortic Nipple-Left SuperiorIntercostal Vein
Aortic Nipple-Left SuperiorIntercostal Vein
The End