
Fractures and Dislocations of the Cervical Spine
Fractures and Dislocations of the Cervical Spine
© William Herring, MD, FACR
3 rules of 3
The predentate space should be < 3mm
The prevertebral soft tissue at C3 isusually 3 mm
Anterior wedging of 3mm or moresuggests a fx
3 rules of 3

Atlanto-axial Dislocation
Hyperextension injury
Children>adults
Head slips forward on C1
Usually fatal

Neural Arch Fracture of C1
Most common fracture of C1
Hyperextension injury
Not associated with neurologic deficit
Confused with congenital anomaly

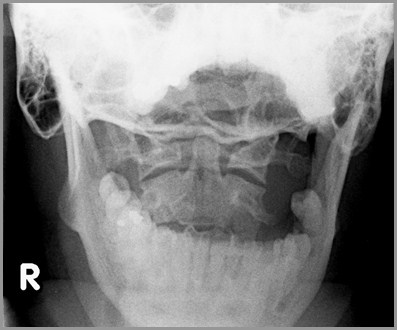
Jefferson Fracture of C1
Burst fracture
Caused by compressive force
Bilateral breaks in anterior and posteriorarches
Open mouth view shows bilateral offset ofC1 on C2
Not associated with neurologic deficit

Hangman’s Fracture of C2
Most common fracture of C2
Most common cervical spine fracture
Hyperextension/compression fracture
Fractures through the pedicles of C2 withanterior slip of C2 on C3
Not associated with neurologic deficit
Teardrop fracture of inferior aspect of C2or C3 is clue to dx of Hangman’s fx


Dens Fractures
Hyperextension injuries
Most associated with forwardsubluxation of C1 on C2
High incidence of non-union (60%)
Stable
Dens FracturesTypes
Tip of densRare (5%)
Base of densCommon (65%)
Sub-dentateUncommon (30%)

Mach line
Congenital non-union
Non-union of previous fracture
Dens FracturesPitfalls in Diagnosis
Dens FracturesPitfalls in Diagnosis
Flexion-Teardrop Fracture
Combination of flexion and compression,e.g. MVA
Teardrop fragment comes fromanteroinferior aspect of body
Remainder of body displaced backwardinto spinal canal
Flexion-Teardrop Fracture
Facet joint and interspinous distancesusually widened
Disk space may be narrowed
70% have associated neurologic deficit
Flexion-Teardrop Fracture

Simple Compression Fracture
Flexion injury
Anterior wedging of 3mm or moresuggests fracture
Usually involves superior endplate ofvertebral body
Simple Compression Fracture

Clay-Shoveler’s Fracture
Avulsion fracture of spinous process ofC6 or C7
Occurs as result of rotation of trunkrelative to neck
No neurologic deficit
Clay-Shoveler’s Fracture

Ligamentous Injuries
Mechanism is flexion/distraction
Disk space narrower anteriorly thanposteriorly
Widening of the interspinpous distance
Widening of the facet joint
Usually the posterior aspect
Ligamentous Injuries
Subluxation of vertebral body
Perched facet
Locked facets
At least 50% subluxation
85% neurologic deficits with locked facets
Ligamentous Injuries

Unilateral Locked Facets
Mechanism is flexion/distraction androtation
Only 30% associated with neurologicdefect
On lateral, some bodies appear lateral,some oblique
Spinous processes do not line up onfrontal film
Unilateral Locked Facets

Bilateral Locked Facets

Unstable Fractures
Jefferson fracture
Hangman’s fracture
Flexion teardrop fracture
Extension teardrop fracture
Bilateral locked facets