|
|
Pulmonary Alveolar Proteinosis
PAP
- General Considerations
- Rare disorder of unknown etiology
- Alveoli are filled with PAS-positive proteinaceous material derived from surfactant phospholipids and proteins
- Males are affected 4X more than females; the disease is most common from 20-50 years of age
- It may be primary or secondary (to pulmonary infections, inhalation of silica or insecticides and hematologic malignancies)
- Diagnosis is usually made by lung biopsy
Clinical Findings
- Almost 1/3 may be asymptomatic even with abnormal chest radiographs
- Symptoms, which are usually gradual in onset, include:
- Dry cough (or scant sputum production)
- Progressive dyspnea
- Fatigue and malaise
- Weight loss
- Intermittent low-grade fever and/or night sweats
- Pleuritic chest pain
- Rarely cyanosis or hemoptysis
Imaging Findings
- Bilateral perihilar consolidation in a configuration which may mimic pulmonary edema, but without cardiomegaly or pleural effusions
- Occasional unilateral; lymphadenopathy is rare
- Typically, changes progress over weeks to months into a diffuse reticulogranular pattern
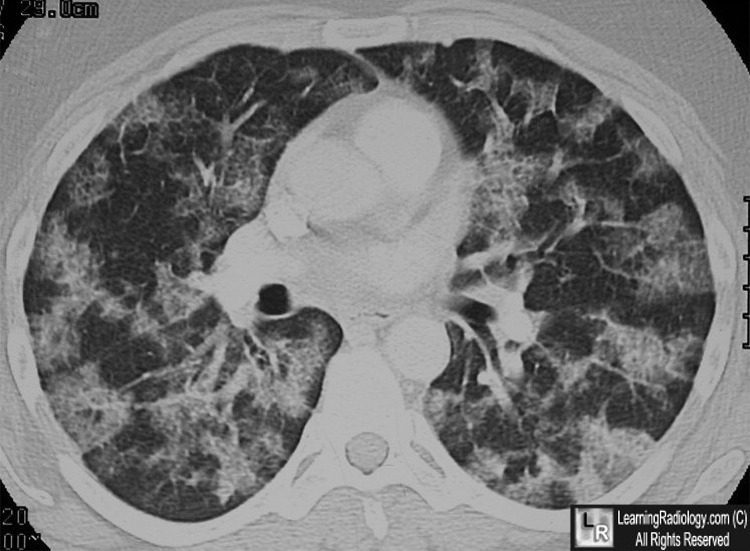
- On CT
- Areas of patchy ground-glass opacification with smooth interlobular septal thickening and intralobular interstitial thickening ® a polygonal pattern referred to as "crazy paving"
- DDX for “crazy paving:” exogenous lipoid pneumonia, sarcoidosis, mucinous bronchoalveolar cell carcinoma, and acute respiratory distress syndrome
Differential Diagnosis
Treatment
- Usual care for PAP is mechanical removal of the lipoproteinaceous material by whole-lung lavage.
- Historically, systemic steroids have been used, as well as mucolytics (aerosol), and proteinase (aerosol) but without much success.
- Hyperbaric chamber or extracorporeal membrane oxygenation (ECMO) has been used to perform whole-lung lavages in cases of severe hypoxemia
Complications
- Major complications are pulmonary infections with N asteroides, Pneumocystis carinii, and/or mycobacterium avium intracellulare
- Pulmonary fibrosis and/or cor pulmonale also can complicate PAP.
- Some association between anti-GM-CSF autoantibodies and some cases of cryptococcal meningitis in otherwise immunocompetent patients.
Prognosis
- The mortality rate is reported to be under 10%
- The mortality rate of secondary PAP depends on the underlying disease

Pulmonary Alveolar Proteinosis. There are areas of patchy ground-glass opacification with smooth interlobular septal thickening and intralobular interstitial thickening (white circles) a polygonal pattern referred to as "crazy paving"
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
XXXXX
|
|
|

{kind=link}
{kind=link}