|
|
Hodgkin Disease
General Considerations
- Half of patients with Hodgkin have mediastinal lymph node enlargement visible on chest x-ray.
- About 5-10% of patients may have mediastinal adenopathy without any other nodes involved
- Clinically, over 90% of patients with Hodgkin have enlarged nodes, the disease behaving most benignly when restricted to the neck
- Most have nodular sclerosing type
Types |
Classified As |
Nodular sclerosis |
Hodgkin lymphoma |
Mixed cellularity |
Hodgkin lymphoma |
Lymphocyte depleted |
Hodgkin lymphoma |
Lymphocyte rich |
Hodgkin lymphoma |
Nodular lymphocyte predominant Hodgkin disease (NLPHD) |
Distinct entity -- unique clinical features, different treatment |
Clinical Findings
- Most patients with disease above diaphragm are asymptomatic
- “B” symptoms are present in 40%
- Unexplained weight loss
- Fever
- Night sweats
- Intermittent fever in about 35% of cases
- Infrequently, Pel-Ebstein fever (high fever for 1-2 wk followed by an afebrile period of 1-2 wk)
- A large mediastinal mass may produce chest pain, cough or shortness of breath
- Pruritus
- Nodal pain, especially if preceded by drinking alcohol may occur in less than 10% of patients but is characteristic of Hodgkin lymphoma
- Rarely, hemoptysis
- Rarely, back or bone pain
Imaging Findings
- Parenchymal lung involvement occurs in 1/3 of patients with Hodgkin
- Almost all have associated hilar or mediastinal adenopathy
- Most common manifestation
- Present in 90-99%
- Commonly multiple lymph node groups involved
- Anterior mediastinal and retrosternal nodes commonly involved
- Confined to anterior mediastinum in 40%
- 20% with mediastinal nodes have hilar lymphadenopathy also
- Hilar lymph nodes involved bilaterally in 50%
- Bronchovascular form (most common type of involvement)
- Coarse reticulonodular pattern contiguous with mediastinum from direct extension from mediastinal nodes along lymphatics
- Nodular parenchymal lesions
- Miliary nodules
- Endobronchial involvement
- Lobar atelectasis secondary to endobronchial obstruction (rare)
- Atelectasis is very uncommon and almost always due to an endobronchial lesion
- Cavitation secondary to necrosis (rare)
- Subpleural form
- Circumscribed subpleural masses
- Pleural effusion from lymphatic obstruction
- About 1/3 have pleural effusions
- Effusion usually does not contain malignant cells
- Pneumonic form
- Diffuse nonsegmental infiltrate (pneumonic type)
- Massive lobar infiltrates (30%)
- Homogeneous confluent infiltrates with shaggy borders
- Nodular form
- Multiple nodules <1 cm in diameter
- Extraparenchymal manifestations in the chest
- Hilar adenopathy is usually bilateral but asymmetric
- Anterior mediastinal nodes commonly involved
- They may calcify after radiation therapy
Staging (Ann Arbor)
- Stage I is adenopathy limited to one lymph node bearing group
- Stage II is adenopathy involving two or more non-contiguous groups on the same side of the diaphragm
- Stage III is adenopathy involving lymph node groups on both sides of the diaphragm
- Stage IV is extranodal involvement-such as lung or brain
- Other modifiers
- S – Splenic involvement
- B – Presence of B symptoms (temperature >38°C, drenching night sweats, unexplained loss of >10% of body weight in the preceding 6 months)
- A – Absence of B symptoms
- X – Presence of bulky disease
- E – Contiguous involvement of extranodal sites
Differential Diagnosis
- Sarcoid
- Primary tuberculosis
- Bronchogenic carcinoma, especially small cell
Treatment
- Radiation therapy is generally administered in combination with chemotherapy in classic Hodgkin Disease
- Thoracic radiation portal is called a “mantel” because of its T shape to cover supraclavicular and mediastinal nodes
- Lymphoma is radiosensitive – tumors frequently beginning to show reduction in size almost at once
Prognosis
- Prognostically, mediastinal node enlargement worsens prognosis but only minimally.
- Diffuse lung involvement, on the other hand, carries a graver prognosis
Five-year Survival Rates for Hodgkin Lymphoma |
Stages I and II |
90% |
Stage III |
84% |
Stage IV |
65% |


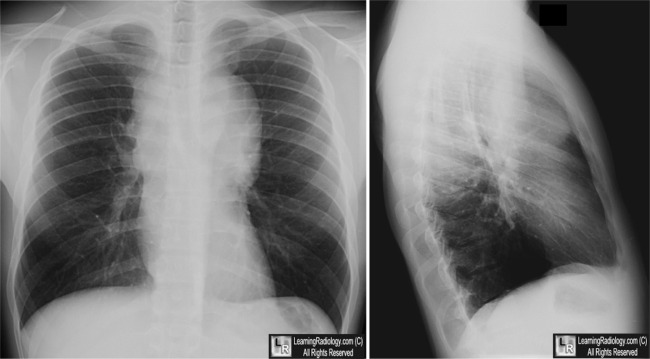
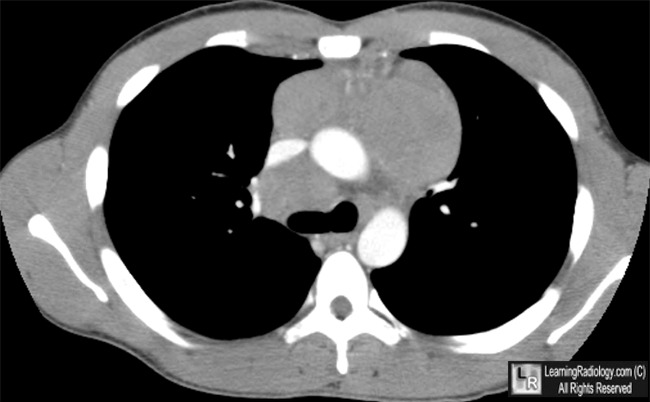
Hodgkin Disease. Upper: Frontal and Lateral radiographs of the chest show large, bulky, lobulated soft tissue masses in the mediastinum (white arrows). Lower: Axial contrast-enhanced CT scan of the chest again demonstrates massive mediastinal soft tissue masses consistent with lymphoma (white arrows).)
For this same photo without the arrows, click here and here
For more information, click on the link if you see this icon 
Hodgkin Lymphoma. BW Lash, SK Dessain,and A Argiris. eMedicine
|
|
|

{kind=link}
{kind=link}