|
|
Thymoma
General Considerations
- Most common anterior mediastinal neoplasm
- Mean age of presentation is 52, older than teratomas
- Most are solid lymphoepithelial tumors of the thymus, some are cystic
- About 1/3 are malignant
- Rare in children — most common around 5th or 6th decade
- Four types which occur in about equal frequency
- Lymphocytic
- Epithelial
- Mixed
- Spindle cell (Hassall’s corpuscles in this type)
- About 15% of patients with myasthenia gravis have follicular thymic hyperplasia and about 50% of patients with follicular thymic hyperplasia have myasthenia
- Other associated disorders include: red cell aplasia, dermatomyositis, systemic lupus erythematosis, Cushing syndrome, and syndrome of inappropriate antidiuretic hormone secretion
Clinical Findings
- 1/3 to ½ are asymptomatic
- About 1/3 present with local symptoms
- Cough
- Chest pain
- Superior vena caval syndrome
- Dysphagia
- Hoarseness
- About 1/3 are found during workup for myasthenia gravis
Imaging Findings
- Oval round or lobulated soft tissue mass, sharply demarcated, usually smaller than teratomas
- Usually occur in upper third of chest around the heart and great vessels, which they may displace posteriorly
- Thymomas may spread along pleural reflections to posterior mediastinum, diaphragm and retroperitoneum
- CT is the study of choice in detecting enlarged thymus in patients with myasthenia gravis
- Small tumors may show homogeneous enhancement; larger tumors are usually heterogeneous
- Larger tumors especially may show cystic areas and necrosis
- Invasive thymoma may demonstrate unilateral pleural nodules or masses, mimicking pleural metastatic disease or mesothelioma
- About 30% may contain curvilinear or, less commonly, amorphous calcification
- Look for invasion of adjacent vessels or pericardium (thickening)
Differential Diagnosis
- Teratoma – occurs in younger age group; may contain bone and fat

- Lymphoma
- Thymolipoma
- Fatty tumors of the thymus which constitute 2-9% of thymomas
- They can grow to huge sizes
Treatment
- Surgical resection
- If unresectable, chemotherapy is frequently used
Prognosis
- Surgical evaluation of encapsulation or invasion is better indicator of malignancy than actual histology
- In patients with myasthenia, about 50% improve following removal of the thymic tissue
- Recurrence rate can be high (50% 10 year survival)
- Thymomas are associated with second malignancies, especially non-Hodgkin lymphoma


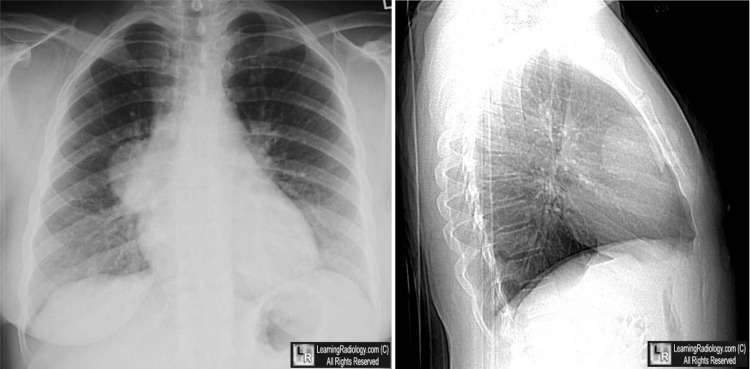
Thymoma. Upper: Frontal and lateral views of the chest show a well-circumscribed anterior
mediastinal mass without apparent calcifications (white and black arrows).
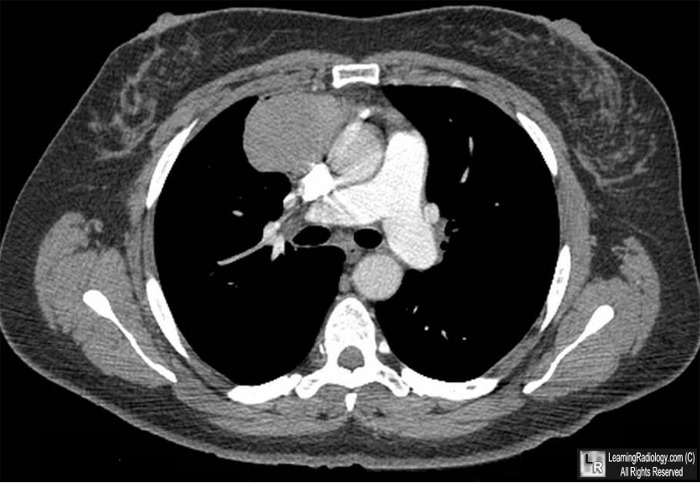
Lower:Axial CT scan of the upper chest shows a non-enhancing lobulated but sharply marginated
anterior mediastinal mass (yellow arrow)..
For these same photos, click here and here
For more information, click on the link if you see this icon
Thymoma. KJ Evans, Q Miller, and AL Kline. eMedicine
|
|
|

{kind=link}
{kind=link}