|
|
Necrotizing Enterocolitis
General Considerations
- Most common gastrointestinal medical and/or surgical emergency occurring in neonates
- Etiology
- Remains unknown
- Ischemia and/or reperfusion injury may play a role
- Cluster cases and outbreaks in nurseries imply an infectious etiology
- A single causative organism has not been found
- Translocation of intestinal flora across compromised mucosa may play a role
- Incidence and age at onset
- More common in premature infants
- But can also be seen in term babies
- Inversely related to birth weight and gestational age
- Term infants develop NEC earlier after birth than preemies
- Average age of onset occurs within first week of life
- Affected term neonates are usually systemically ill with other conditions such as birth asphyxia, respiratory distress or congenital heart disease
- Premature babies are at risk for several weeks after birth
- Babies who are breastfed have a lower incidence of NEC than formula-fed babies
Clinical findings
- Initial symptoms may be subtle and can include the following
- Feeding intolerance
- Delayed gastric emptying
- Abdominal distention and/or tenderness
- Ileus/decreased bowel sounds
Imaging findings
- Acute disease most commonly affects the terminal ileum
- Plain film of the abdomen remains method in which disease is diagnosed most often
- Findings include
- Dilated loops of bowel
- Thickened bowel walls
- Fixed and dilated loop that persists is especially worrisome
- Absence of bowel gas
- Pneumatosis intestinalis
- Pathognomonic of NEC in newborn
- Linear radiolucency parallels bowel lumen within bowel wall
- Represents air that has entered from the lumen
- Abdominal free air
- Ominous
- Usually requires emergency surgical intervention
- May require a left lateral decubitus view to be seen
- Portal venous gas
- Originally thought to be ominous but is now considered less so
- Appears as linear branching areas of decreased density over periphery of the liver
- Represents air in portal venous system
- Ascites
- Late finding
- Develops after perforation when peritonitis is present
Complications
- Occur in about 75% of all patients survive
- Of those who survive, 50% develop a long-term complication
- Two most common complications are intestinal stricture and short-gut syndrome
- Intestinal strictures
- Can develop in infants with or without a preceding perforation
- Incidence is 25-33%
- Strictures most commonly involve the left side of the colon
- Diagnosed with barium enema
- Short-gut syndrome
- Malabsorption syndrome resulting from removal of excessive or critical portions of small
- Neonatal gut will grow this growth may take as long as 2 years to occur
Mortality
- Mortality rate ranges from 10-44% in infants weighing less than 1500 g


Necrotizing Enterocolitis. Upper photo: There are multiple dilated loops of bowel (yellow arrow).
A linear radiolucency is seen paralleling the bowel wall indicating air in the wall (white arrow).
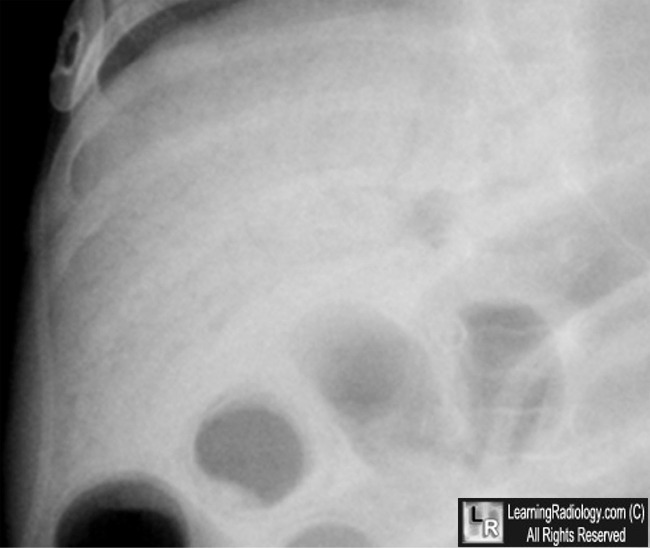
There is air in the portal venous system (blue box, see close-up below).
Lower photo: Close-up view of the liver shows multiple branching, air-containing venous structures
extending to the periphery of the liver (yellow circle)
For this same photo without the arrows, click here and here
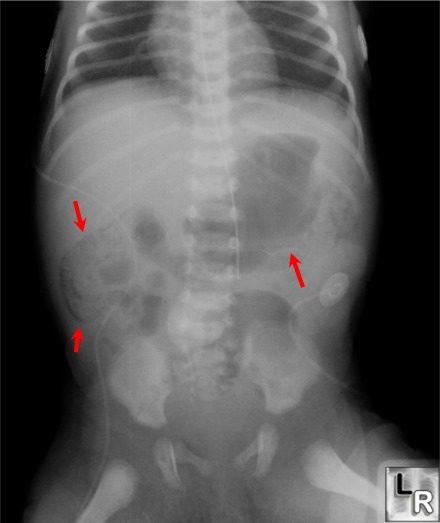
Red arrows point to
linear bands of radiolucency which parallel
the wall of the
bowel indicating the presence of pneumatosis
intestinalis in necrotizing enterocolitis
For more information, click on the link if you see this icon 
eMedicine.com: Necrotizing Enterolcolitis; Shelley C Springer, MD, MBA, MSc, and David J Annibale, MD
|
|
|

{kind=link}
{kind=link}