|
|
Pancoast Tumor
Superior Sulcus Tumor
General Considerations
- A lung tumor arising in the superior sulcus and comprising fewer than 5% of all primary lung cancers
- Described by Henry Pancoast in 1932
- The majority of the tumor growth is extrathoracic
- Directly invades
- Adjacent ribs, especially the 1st, 2nd and 3rd
- Vertebrae
- Brachial plexus
- Stellate ganglion
- Most are squamous cell carcinomas
- Fewer than 5% are small cell carcinomas
Clinical Findings
- Shoulder pain is most common presenting symptom
- From extension to brachial plexus, vertebral bodies, pleura or ribs
- Pain radiates along ulnar nerve distribution to the hand
- Muscle weakness, atrophy and parasthesia
- Horner’s syndrome in up to 50% due to invasion of the superior cervical sympathetic chain and stellate ganglion
- Superior vena caval obstruction
- Phrenic and recurrent laryngeal nerve involvement
- Rarely, they may produce paraneoplastic syndromes ranging from Cushing’s to inappropriate secretion of antidiuretic hormone
Imaging Findings
- MRI is probably more sensitive than CT in identifying extension of the tumor into adjacent soft tissues and bone
- Frontal chest radiographs show
- Unilateral apical soft tissue mass
- Sometimes the mass can be very flat and plaque-like
- It may be difficult or impossible to see on initial radiographs
- Local rib destruction is highly suggestive
- Occasionally, an AP radiograph of the cervical spine is better at demonstrating the tumor and associated rib destruction than a conventional chest radiograph
- Apical lordotic films of the chest may also be helpful
- CT scans may assist in evaluating
- Bone destruction
- Mediastinal adenopathy
- Presence of other pulmonary nodules and liver
Differential Diagnosis
- Tuberculosis
- Plasmacytoma
- Mesothelioma
- Subclavian artery aneurysms
Treatment
- Diagnosis is usually made by trans-thoracic needle biopsy
- Because of their location, bronchoscopy is frequently not able to reach tumor
- Invasion of adjacent vertebral body, the spinal canal or the upper brachial plexus as well as distant metastases are contraindications for surgery
- Preoperative radiation therapy followed by surgical resection is the most common form of treatment
Complications
- Surgical complications include
- Chest pain
- Spinal fluid leaks
- Horner’s syndrome
Prognosis
- Most tumors are Stage III at diagnosis
- Overall 5 –year survival is around 30%
- Right-sided Pancoast tumors have a worse 5-year survival than left-sided lesions
 
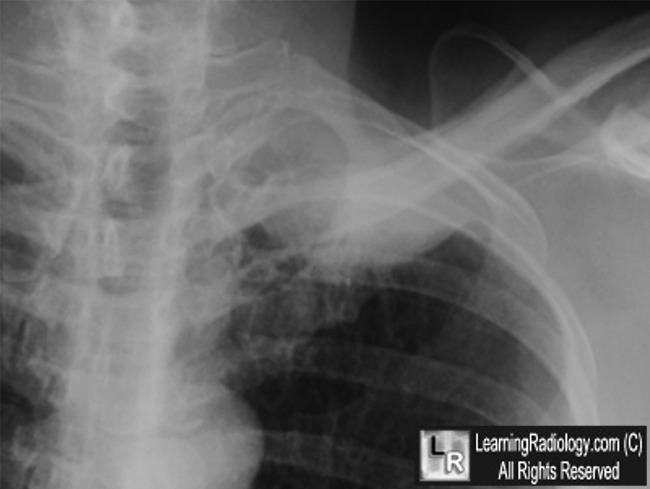
Pancoast Tumor. Frontal chest radiograph demonstrates a mass in the left lung apex
(white arrow in left image). There is associated destruction of the left 2nd and 3rd ribs posteriorly (white circle). The close-up photo of the left apex shows the rib destruction (white arrow) more clearly. The combination of an apical mass with rib destruction
is characteristic for a Pancoast Tumor.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
Pancoast Tumor eMedicine Melanie Guerrero, MD, Shabir Bhimji, MD.
|
|
|

{kind=link}
{kind=link}