|
|
Aspiration
General Considerations
- Aspiration represents material that passes through the true vocal cords into the trachea
- Predisposing factors
- Stroke
- Dementia
- Multiple sclerosis
- Parkinson’s disease
- Myasthenia gravis
- GERD
- Prior head and neck irradiation
Normal Phases of Swallowing Function and Swallowing Disorders |
Phase |
Description |
Abnormalities |
Oral |
Chewing and manipulating food/liquids in the mouth.
Conversion of food from solid to semisolid.
Requires intact dentition and is negatively affected by poor salivary gland function (lubrication), surgical defects, and neurologic disorders. |
Holding of food in mouth, circumoral leakage, and early pharyngeal spill from weakness and poor coordination of the lips, cheeks and tongue.
Aspiration of food before pharyngeal swallowing due to premature pharyngeal spill.
Weak posterior tongue ® abnormal tongue thrusting.
Changes in mental status with cognitive deficits can affect initiation of swallowing, increasing tendency to pocket food in the lateral sulci ® possible aspiration. |
Pharyngeal |
Shortest phase and most complex.
Soft palate elevates closing off nasopharynx and preventing nasopharyngeal regurgitation. Superior constrictor muscle contracts.
Pharyngeal peristalsis begins while tongue base drives bolus posteriorly.
Respiration ceases during expiration-the larynx elevates and epiglottis retroflexes, driving bolus around opening of larynx.
Arytenoids adduct and are approximated to the base of epiglottis.
Bolus propulsion enhanced by passive and active dilatation of upper esophageal sphincter (of which cricopharyngeus is part).
Cricopharyngeal and inferior constrictor muscles then relax, allowing food to pass into upper esophagus. |
Dysfunction or abnormalities of soft palate and superior pharynx ® nasopharyngeal reflux.
Defect in thyrohyoid and palatopharyngeal muscle function and hyoid bone elevation ® reduced laryngeal and pharyngeal elevation, resulting in aspiration.
Pharyngeal constrictor weakness ® accumulation of food residue in valleculae and piriform sinus (pooling) which could be aspirated after swallowing.
Impaired relaxation, distensibility, fibrosis, hyperplasia, or hypertrophy of cricopharyngeus muscle ® improper coordination of swallowing. |
Esophageal |
Bolus is propelled about 25 cm from cricopharyngeus through thoracic esophagus via peristaltic contractions.
Lower esophageal sphincter relaxes and bolus moves into gastric cardia. |
Achalasia ® reduced gastroesophageal junction relaxation or absent esophageal peristalsis.
Zenker diverticulum ® swallowing difficulty, possibly with nocturnal aspiration of residue in tic.
Other defects in wall of esophagus or in external structures (eg, in hilar lymph nodes) ® dysfunction in propulsion of bolus from esophagus to stomach (eg, esophageal webs, rings) resulting in weak esophagopharyngeal peristalsis due to scleroderma or other conditions. |
eMedicine. Swallowing Disorders. ST Dawodu |
Clinical Findings
- Cough after swallowing or drinking
- Aspiration can occur in the absence of cough (silent aspiration)
- Especially prone to occur in neurologically impaired individuals and those with other GI problems
- Dysphagia
- Recurrent pneumonia
- Drooling
- Nasal regurgitation
- Dehydration
- Malnutrition
- Unintentional weight loss
Imaging Findings
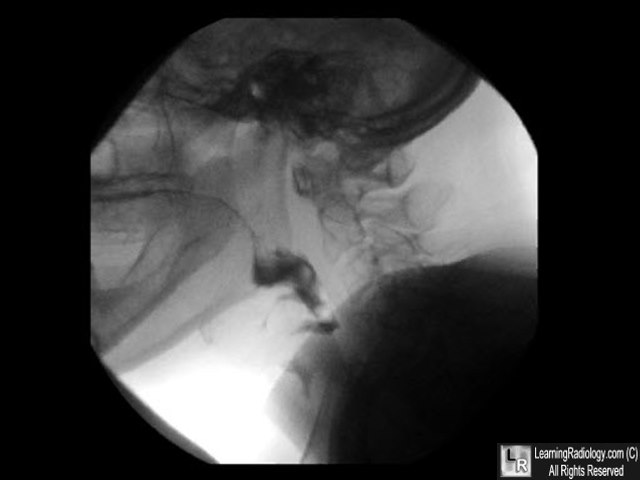
- Video fluoroscopic swallowing examination (aka modified barium swallow)

- Performed under supervision of speech-language pathologist and radiologist
- Puree, liquid, and/or solid consistency barium is administered in varying amounts while fluoroscopic image (lateral and anterior-posterior) is recorded digitally or on videotape
- Another means of assessing penetration/aspiration is the fiberoptic endoscopic evaluation of swallowing (FEES)
- Contrast passes through the glottis below the level of the true cords into the trachea
- The patient may or may not cough in response
- Contrast may remain in the trachea or may be expelled with the patient’s cough
Differential Diagnosis
- In penetration, barium enters laryngeal vestibule but does not pass below the level of glottis
Complications
- Aspiration pneumonia is most common form of hospital-acquired pneumonia among adults
Treatment
- Goals of focus on reduction of aspiration, improved swallowing ability in order to optimize nutritional status
- Patients with dysphagia are usually managed by multidisciplinary teams that may include a physician, a nurse, a speech language pathologist, a dietitian, and physical and occupational therapists
- Some treatments used may include:
- Recommendations for liquid consistency intake (consistency modifications)
- Physiologic exercise programs to strengthen swallowing musculature –chin tuck, head rotation, head tilt
- Pharmacologic treatment with angiotensin-converting enzyme (ACE) inhibitors for pneumonia and aspiration has been reported in the elderly and patients with stroke
- Surgeries for intractable aspiration include such radical procedures as laryngectomy and tracheostomy, and conservative procedures which preserve speech and swallowing functioning
Prognosis
- When recovery is possible (eg, stroke), it may take from 3 weeks to approximately 6 months or longer for swallowing function to return to normal
- In stroke patients, swallowing dysfunction after 6 months is associated with increased morbidity and mortality

Aspiration. A static image from a video swallowing function study shows barium
has passed beneath the epiglottis (red arrow) and is well below the level of the glottis in the trachea (white arrow).
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Laryngeal Penetration and Aspiration During Swallowing After the Treatment of Advanced Oropharyngeal Cancer. MB Gillespie; MB Brodsky; TA Day; AK Sharma; F Lee; B Martin-Harris. Arch Otolaryngol Head Neck Surg. 2005;131:615-619
Cough and Aspiration of Food and Liquids Due to Oral-Pharyngeal Dysphagia
ACCP Evidence-Based Clinical Practice Guidelines. CA Smith Hammond and LB Goldstein. Chest.129.1_suppl.154S CHEST January 2006 vol. 129 no. 1 suppl 154S-168S.
|
|
|

{kind=link}