|
|
Dermoid of Skull
Epidermoid Inclusion Cyst
General Considerations
- Benign, slow-growing tumors of the skull (“cyst” and “tumor” are used interchangeably)
- Believed to occur secondary to aberrant epidermal or dermal inclusion in the calvarium
- Although rare, it is still , along with Langerhans cell histiocytosis, one of the more common lesions in the pediatric skull
Clinical Findings
- Most often present between 20-40 years of age, dermoids slightly earlier than epidermoids
- Painless subcutaneous swelling is most common presentation
- If large enough, they can compress cranial nerves
Imaging Findings
- Intradiploic
- Well-demarcated lytic lesions which tend to expand both the inner and outer tables and demonstrate sclerotic borders
- Epidermoid cysts occur in bones of the skull in this order of frequency
- Frontal bone
- Occipital bone
- Orbit
- Dermoid cysts tend to be midline in the frontotemporal and then parietal locations
- Most involve the course of a suture line near the anterior fontanelle
- On CT, they are hypodense and non-enhancing
- On MRI, they are low intensity on T1 and high on T2
Differential Diagnosis
Treatment
- Surgical removal or curettage
Complications
- May communicate with sinuses
- Rarely may become infected
- Rarely may involve underlying dural sinuses
- Associated with Klippel-Feil syndrome
Prognosis


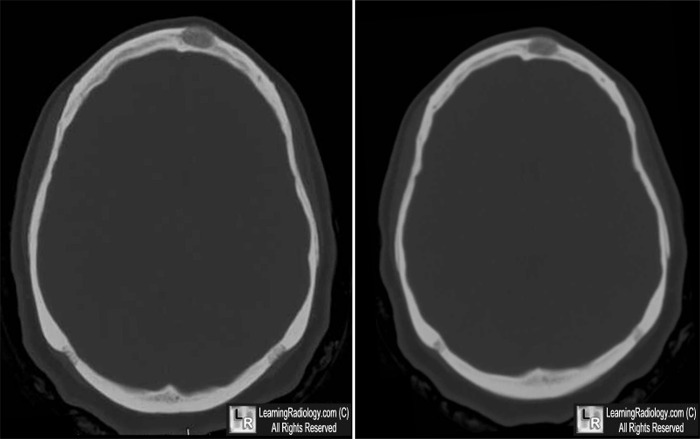
Dermoid Cyst of the Skull. Top. Well-demarcated, lytic lesion of the diploic space (white arrows) expanding the
outer table adjacent to the midline. Lower. Same lesion as seen on the scout image of the CT (yellow arrow)
is seen in the frontal bone expanding the diploic space.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
SE Gibson and RA Prayson. Primary Pediatric Skull Lesions. Arch Pathol Lab Med: Vol 131, May 2007
|
|
|

{kind=link}
{kind=link}