|
|
Pacemaker Lead Perforation
General Considerations
- Perforation can occur during placement (more frequent) or delayed (up to 5 years after implantation)
- Cardiac tissue has a "self-sealing" capacity
- Incidence of around 1% for pacemakers and 1-5% for cardiac defibrillators
- Probably more common than originally thought
- Risk factors for cardiac perforation
- Heart wall thickness
- Use of oral steroids within 1 week of implantation
- Age
- Female gender
- Coagulation status
- Body Mass Index less than 20
Clinical Findings
- Twitching of the chest wall or diaphragm
- Chest pain and hypotension
- Cardiac tamponade
- Pericarditis, friction rub
- Active fixation leads
Imaging Findings
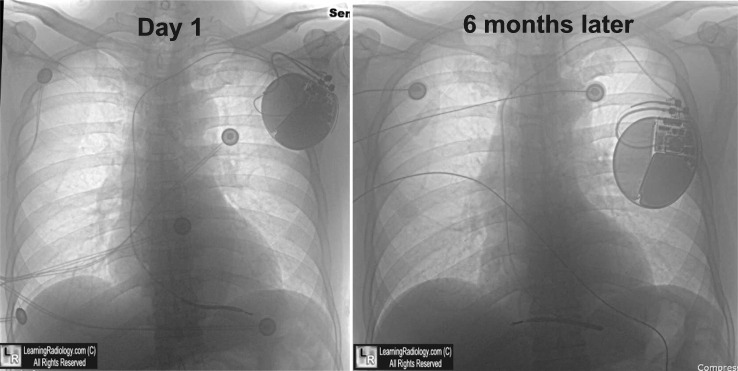
- On chest radiographs, leads should have smooth curves and do not usually change in position over time
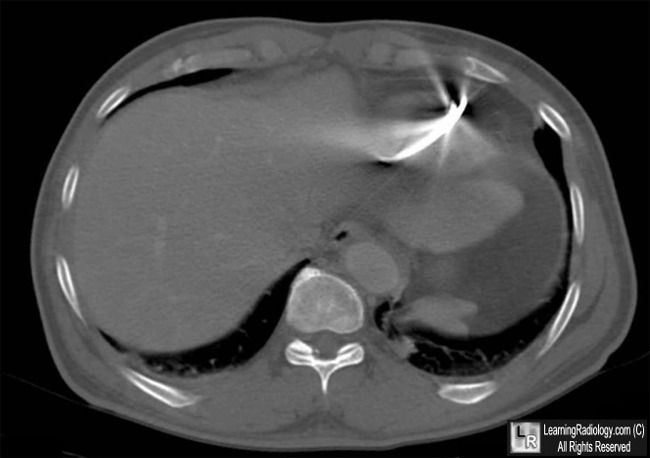
- CT is the study of choice
- Hemopericardium may or may not occur
Treatment
- If the perforation is associated with hemodynamic instability, emergency treatment is usually required
- Extraction may be done, monitoring for pericardial bleeding
- Atrial perforations are less likely to self-seal as are ventricular perforations


Pacemaker Lead Perforation. (Chest radiographs are shown with black and white reversed to better show abnormality) The position of the right ventricular lead is shown (white arrow) on insertion
of the pacemaker. Several months later, the position of the lead has changed (red arrow)
and the lead is now kinked. A CT scan of the chest at the level of the diaphragm
demonstrates the lead resides outside of the myocardium on the under surface of the heart (blue arrow)..
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
Implantable Pacing Leads and Risk of Cardiac Perforation. Boston Scientific Advisory. September, 2007
|
|
|

{kind=link}
{kind=link}