|
|
Skull Flap Implanted in Abdominal Wall
General Considerations
- On occasion, a portion of the skull may be emergently removed to relieve increased intracranial pressure (decompressive craniectomy)
- Mostly performed for acute subdural hemorrhage
- The remaining dura mater may be sewn together and the patient may wear a protective helmet
- Although other materials can be used to replace the bone flap, sometimes the patient's own skull flap is preserved for re-use
- Cosmetically, this can provide the best result
- The bone flap can be frozen, stored in sterile solutions or sewn into the subcutaneous tissue of the patient's abdomen where its viability is maintained by the body
- Advantages of storing the bone flap in the abdominal wall include sterility and continued nourishment that allows for the chondroblasts and osteoblasts to mature
- The flap is returned to the skull typically in 6-20 weeks after removal
Clinical Findings
- History of recent decompressive craniectomy or hemicraniectomy
Imaging Findings
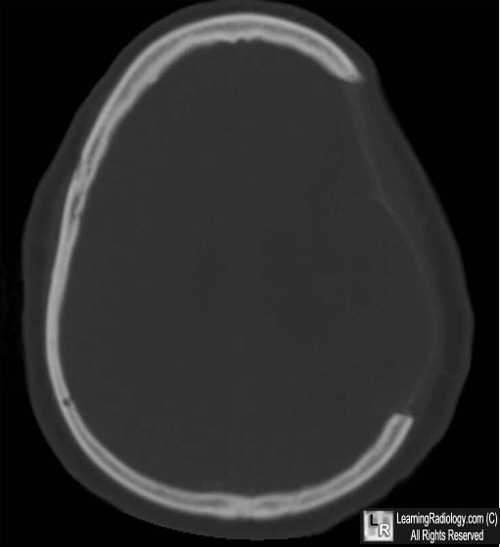
- Absence of a portion of the skull from the cranial vault
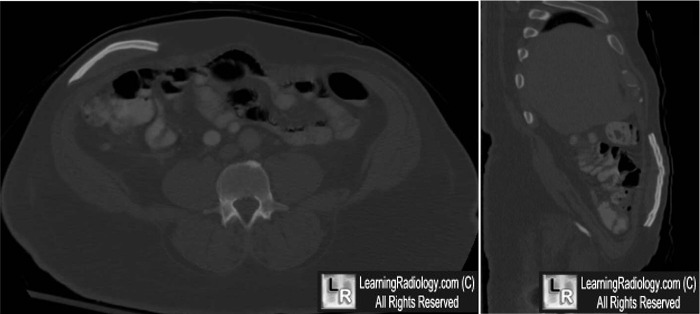
- Presence of a bone flap in the anterior abdominal wall with the typical appearance of the inner and outer tables of the skull
Differential Diagnosis
Complications


Skull flap implanted in abdominal wall. There is a skull flap seen in the right anterior abdominal wall
(white arrows) on this axial and sagittally re-formatted CT of the abdomen using bone windows.
The flap was removed during a decompressive craniectomy from the right parietal region (yellow arrow)
and stored in the abdominal wall for re-implantation.
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here and here
Skull Cap in Anterior Abdominal Wall. Steven H Craig. USUHS.
Cranioplasty: why throw the bone flap out?. Flanndry T; McConnell RS. British Journal of Neurosurgery, 2001; 15(6): 518-520.
|
|
|

{kind=link}
{kind=link}