|
|
Sinus of Valsalva Aneurysm
Ruptured Sinus of Valsalva Aneurysm
General Considerations
- Usually congenital
- 65-85% of SVAs originate from the right sinus of Valsalva
- Noncoronary (10-30%)
- Left sinuses (<5%) are very rare
- Congenital most often from single sinus
- Secondary causes more often include the left sinus and include
- Endocarditis of aortic valve
- Syphilis
- Atherosclerosis
- Dissecting aneurysm
- Marfan's syndrome
- Male-to-female ratio is 4:1, ruptured and unruptured
Clinical findings
- Unruptured SVA is usually asymptomatic and found serendipitously
- May be a cause of heart block from compression of conducting system
Imaging findings
- Cine MRI is the study of choice although most lesions can be seen with 2D or 3D echocardiography
- Since aortic root is intracardiac, usual aneurysm is not visible
- Rarely, a large aneurysm of left aortic sinus produces bulge on left upper heart border in region of LA appendage
- Rarely, a large aneurysm of the right aortic sinus leads to bulge on right heart border
- Usually the aneurysm dilates the aortic ring which can lead to aortic insufficiency
Complications
- Congenital SVAs may be associated with
- Supracristal or perimembranous ventricular septal defect (30-60%)
- Bicuspid aortic valve (15-20%)
- Aortic regurgitation (44-50%)
- Approximately 10% of patients with Marfan syndrome have some form of SVA
- Rupture
- Rupture of SVA (with progressive heart failure and left-to-right shunting or endocarditis) is the main cause of death and rarely occurs before age 20 years in congenital SVA
- May rupture leading to aortic-cardiac fistula (L to R shunt usually)
- Congenital forms (usually R sided) always produce an intracardiac fistula
- Acquired forms can produce either intra- or extracardiac fistulae
- Aortic sinus (also called anterior or septal sinus) is involved 3/4 time and ruptures into the right ventricle or right atrium (rarely)
- Posterior (non-coronary) aortic sinus is involved 1/4 time, usually into right atrium
- May also rupture into the pericardial space
- Most congenital aneurysms rupture during the third or fourth decade
Treatment
- Surgery is definitive treatment
- Urgent surgical repair for ruptures aneurysms
- Many recommend surgical repair of non-ruptures aneurysms as well
Complications
- Rupture (see above)
- Myocardial infarction
- Heart block
- Right ventricular outflow tract obstruction
- Cardiac tamponade
- Sudden death
Prognosis
- Poor with rupture unless urgent surgical repair
- Most unruptured SVAs progressively dilate and eventually rupture

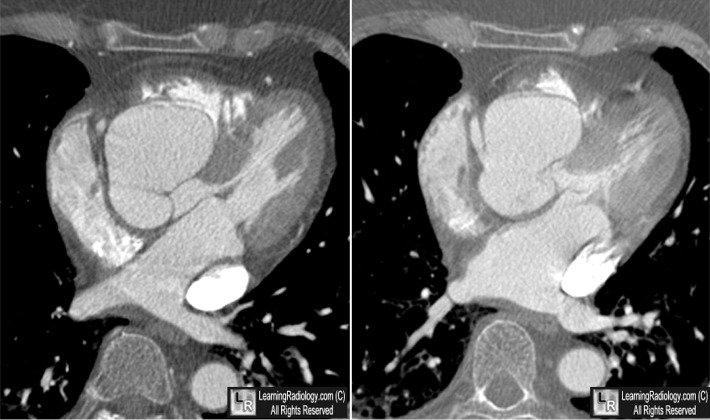
Sinus of Valsalva Aneurysm. Contrast-enhanced axial CT scans through the heart demonstrate an aneurysm (black arrows) of the right coronary sinus (RC) from which the right coronary artery arises (red arrow). The left coronary artery (yellow arrow) arises form the left coronary sinus (LC). The non-coronary sinus is posterior (NC).
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here
Sinus of valsalva aneurysm. Charles White and Gary Plotnick. Radiology 2001; 219:82-85.
|
|
|

{kind=link}