|
|
Renal Tuberculosis
General Considerations
- GU tract second most common site of tuberculous infection after lungs
- Males more commonly infected than females, most often < 50 years old
- Spread is hematogenous and usually occurs with primary exposure
- Although may not be clinically apparent at this time, remaining latent for decades
- Active pulmonary TB seen only 4-8% of time
- Only about 25% of patients with GU TB have a known history of pulmonary TB
- Begins as small tubercle and extends to renal tubules and medulla as necrotizing lesions produce larger cavities which communicate with collecting system
- Stricturing eventually results in a fibrotic and small kidney
- Prostatic TB is from descending infection, unlike involvement of seminal vesicles
Clinical Findings
- Hematuria, microscopic or macroscopic
- Stone formation
- Frequency, dysuria and urgency
- Sterile pyuria
Imaging Findings
- Plain films may show large globular, amorphous calcifications or smaller nondescript stones
- Intravenous pyelography or, more recently, CT urograms can be diagnostic
- Affected kidney may contrast-enhance on CT
- Renal calcification is common (24-44%)
- Stones, focal or extensive globular calcification, ring-like calcifications of papillary necrosis
- Cortical scarring
- "Smudged" papillae (moth-eaten) –irregular due to inflammation and necrosis
- Several cysts surrounding a calyx with cortical thinning
- Infundibular strictures
- Hydrocalyces without dilatation of renal pelvis, or
- Hydronephrosis
- "Putty kidney" – sacs of caseous, necrotic material
- Autonephrectomy – small, shrunken kidney with dystrophic calcification
- Bilateral, but frequently asymmetric
- About 75% unilateral radiologically
- When ureters are involved, usually the upper or lower third (more common)
- Beading (sawtooth ureter), corkscrew, strictures
- Bladder involvement rarely leads to calcification of wall (think schistosomiasis)
- Reflux, thickening of bladder wall (thimble bladder), fistula formation
- On US, findings can include hypoechoic masses with hydronephrosis
Differential Diagnosis
- Chronic pyelonephritis
- Papillary necrosis
- Medullary sponge kidney
- Xanthogranulomatous pyelonephritis
Treatment
- Anti-tuberculous drugs
- Nephrectomy
Complications
- Untreated, end result is autonephrectomy
- Infertility in females
- Sinus and fistula tract formation
Prognosis
- With anti-tuberculous drugs, mortality is low (2%)

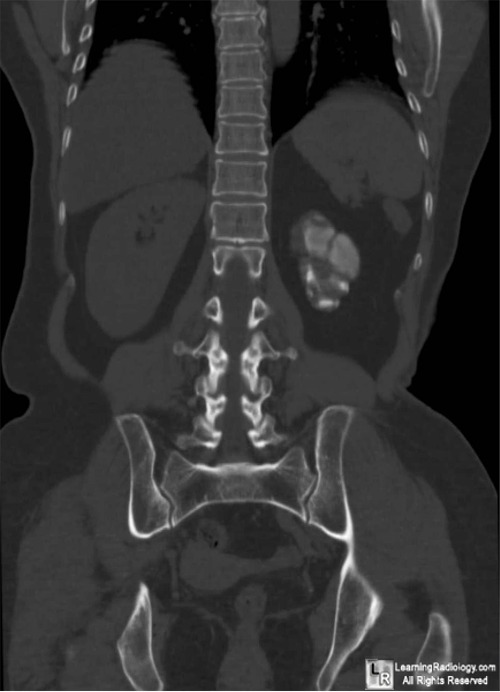
Renal Tuberculosis. Coronal reformatted non-enhanced CT scan of the abdomen and pelvis demonstrates a small, left kidney containing globular calcifications (white circle) pathognomonic for renal tuberculosis.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here
Genitourinary Tuberculosis. eMedicine. Khan, A; Chandramohan, M and MacDonald, S
Renal Tuberculosis. Gibson, M; Puckett, M and Shelly, M. January 2004 RadioGraphics, 24, 251-256.
|
|
|

{kind=link}