|
|
Second Branchial Cleft Cyst
Submitted by Zombor Zoltani, MSIV
General Considerations
- Cystic dilatation of second branchial apparatus
- 95% of all branchial cleft anomalies arise from second cleft of which 75% are cysts
- Other anomalies include fistulas or sinuses or combinations of these
Embryology
- Branchial cleft cysts arise from incomplete obliteration of cervical sinus of His or from buried epithelial cell rests
- Branchial arches are derived from neural crest cells
- Arches are separated by five pairs of grooves and pouches
Clinical Findings
- Typically first appear between 10-40 years of age as painless, compressible, fluctuant, and lateral neck mass
- Neck mass may be chronic and increase in size
- Upper respiratory infections may cause mass to become painful, tender, and enlarge
- Bilateral branchial cleft anomalies occur in 2-3% of cases
Imaging Findings
- Classically, cyst located at anteromedial border of sternocleidomastoid muscle, lateral to carotid space, and at posterior margin of submandibular gland
- May occur anywhere along a line from the oropharyngeal tonsillar fossa to the supraclavicular region of neck
- Beak sign: considered pathognomonic for second branchial cleft cyst
- Represents focal extension of cyst wall superior to internal carotid artery and external carotid artery bifurcation
- Diagnosis made with either CT or MR
- Contrast needed to differentiate cyst from solid mass
CT
- Well circumscribed homogeneously low density cysts with no discernable or very thin wall
- Cyst may be unilocular or septated if secondarily infected
MR
- T1: Isointense to CSF unless secondarily infected then cyst may be hyperintense due to infectious debris
- T2: Hyperintense cyst, minimal wall
Ultrasound
- Anechoic thin walled cyst with posterior acoustic enhancement
- May be hypoechoic or variably echogenic if infected
Differential Diagnosis
- Lymphangioma
- Thymic cyst
- Suppurative jugulodigastic node
- Cystic vagal Schwannoma
- Cystic malignant adenopathy
Treatment and Prognosis
- Complete surgical resection is curative if entire cyst removed
- Inflammation or infection makes surgical resection difficult
- Some cyst associated with fistulas or tracts are challenging to resect


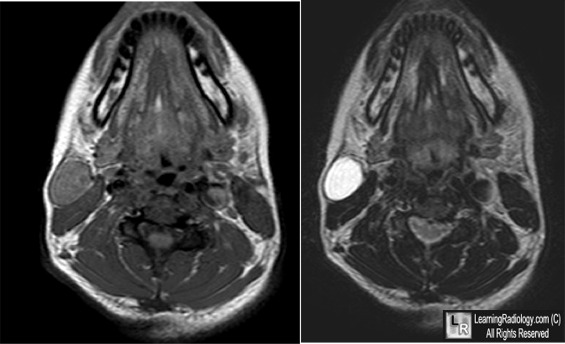
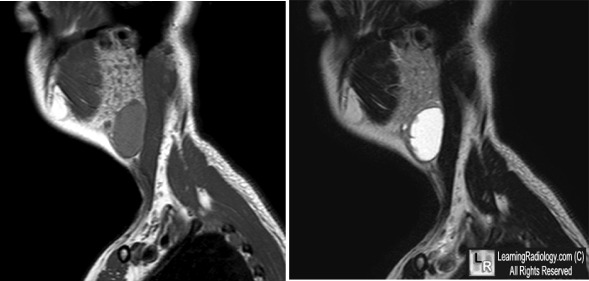
Second Branchial Cleft Cyst. Axial non-contrast MRI images (above) and sagittal contrast-enhanced MRI images below. There is a cystic mass filled with a simple fluid surrounded by a homogeneously enhancing thin-wall in the right neck anteriorly. The cyst is located anterior to the right sternocleidomastoid muscle and inferoposterior to the right parotid gland and is most consistent with a second branchial cleft cyst.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here and here
Harnsberger, Ric H et al. Diagnostic Imaging Head and Neck. Manitoba: Amirsys. 2004.
Koeller Kelly K. et al. From the Archives of the AFIP: Congenital Cystic Masses of the Neck: Radiologic-Pathologic Correlation. Radiographics. 1999; 19: 121-146.
|
|
|

{kind=link}
{kind=link}