|
|
Acute Pancreatitis
- General considerations
- Acute inflammation of the pancreas
- Most commonly caused by alcohol abuse and gallstones
- For reasons not yet fully understood, there is a release of activated pancreatic enzymes into the pancreas and surrounding tissues which causes tissue destruction
- The clinical course of pancreatitis can range from mild (70-80%) to severe (20-30%)
- Most deaths from acute pancreatitis result from sepsis secondary to pancreatic necrosis and infection and multi-organ failure
- Males more often affected than females; 3X more common in African Americans than Caucasians
- Causes
- Gallstones
- Alcohol abuse, usually chronic
- ERCP-induced
- Trauma, more often penetrating
- Drug-induced
- Infectious, especially post-viral in children
- Vasculitis
- Idiopathic
- Clinical findings
- Sudden onset of dull, boring epigastric pain which classically radiates to the back
- Nausea
- Vomiting
- Symptoms frequently begin after heavy drinking or large meal
- Laboratory findings include an elevated serum amylase and lipase levels
- Imaging findings
- Study of choice is contrast-enhanced CT
- Contrast is best for establishing presence of pancreatic necrosis
- Pancreas may appear normal in 25% of patients with mild pancreatitis
- Conventional radiography
- May show colon cut-off sign of air in dilated transverse colon to the splenic flexure
- Localized ileus in left upper quadrant
- May show a paucity of gas from fluid-filled bowel
- Left pleural effusion
- CT
- Focal or diffuse enlargement of the pancreas
- Heterogeneous enhancement
- Indistinct or shaggy margins
- Infiltration of the peripancreatic fat
- Fluid collections in the peripancreatic and anterior pararenal spaces
- MRI
- Used primarily in patients in whom iodinated contrast is contraindicated
- About equal to CT in diagnostic accuracy
- US
- Ultrasound is used primarily for follow-up of pseudocysts or establishing presence of gallstones
- May be helpful in diagnosing a pseudoaneurysm or venous thrombosis
- Complications
- Fluid collections
- Peripancreatic and anterior pararenal space most commonly
- Pseudocyst formation
- Collection of pancreatic juice enclosed by a wall of fibrous or granulation tissue
- Often communicates with the pancreatic duct
- Typically takes about 4 weeks to develop from the onset of clinical symptoms
- Pseudocysts classically appear on CT as a water-density collection with a defined wall which may contrast-enhance
- Abscess
- A circumscribed intra-abdominal collection of pus
- Typically takes about 4 weeks to develop from the onset of clinical symptoms
- May produce a thick-walled fluid collection with gas bubbles or an area of poorly defined fluid with heterogeneous attenuation
- Confirmation of diagnosis may require aspiration of pus
- Pancreatic necrosis
- Focal or diffuse areas of nonviable pancreatic parenchyma, which usually is associated with peripancreatic fat necrosis
- Necrosis typically develops early in course of acute pancreatitis
- Fails to enhance on CT with IV contrast (>3 cm in size)
- Normal, unenhanced pancreas= 30-50 Hu
- Normal enhanced pancreas=100-150 Hu
- Necrosis and abscess may be indistinguishable
- Hemorrhage
- High-attenuation fluid collections
- Venous thrombosis
- Recognized by failure of the peripancreatic veins such as the splenic vein or portal vein to enhance or by the presence of an intraluminal filling defect
- Pseudoaneurysm formation
- Well-defined contrast-containing rounded structure
- Treatment
- Mild pancreatitis is treated medically with IV fluids and analgesics
- In severe cases, treatment may include aggressive fluid therapy, antibiotics and tube feedings
- CT and US can be used for guidance in aspiration of pseudocysts and suspected pancreatic abscesses
- Non-infected pseudocysts resolve spontaneously in about 50% of cases
- Pancreatic necrosis usually requires surgical intervention whereas pancreatic abscesses can be percutaneously drained
- Prognosis
- Overall mortality rate for patients with acute pancreatitis is 10-15%
- With severe disease, rate goes up to 30%

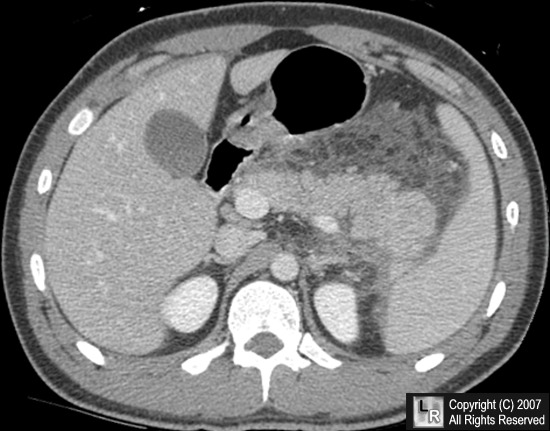
Acute pancreatitis. The pancreas is enlarged (blue arrow) with indistinct and shaggy margins.
There is peripancreatic fluid (red arrow) and extensive peripancreatic infiltration of the
surrounding fat (black arrow).
For more information, click on the link if you see this icon 
For this same photo without the arrows, click here
|
|
|

{kind=link}