|
|
Cystic Nephroma
General Considerations
- Rare, unilateral multi-loculated cystic tumor lacking blastemal elements
- Solitary, well-circumscribed
- Non-communicating fluid-filled locules, surrounded by thick, fibrous capsule
- Do not connect to the collecting system
- Usually quite large (mean 7.6 cm by 9.7 cm)
- Most common in lower pole
- Bimodal occurrence
- Affects males more often in childhood ( 3 months-4 years)
- 50% cystic nephromas and 50% CPDN (see below)
- Females more frequently in adulthood (>30)
Clinical Findings
- Usually presents as a painless flank mass
- Pain
- Hematuria
Imaging Findings
- Ultrasound is the study of choice
- Hydronephrosis is often present due to compression of the mass
- CT
- Multi-loculated cystic mass
- Cysts vary in size
- Septae may enhance
- Heterogeneous
- Calcification is uncommon
- Septae may enhance on MRI following contrast
Differential Diagnosis
- Cystic partially differentiated nephroblastoma (CPDN) is a cystic lesion with blastemal elements
- Anatomically identical to cystic nephroma
- Septae contain blastemal or embryonic cells
- Simple renal cysts
- Cystic renal cell carcinoma
- Enhancing nodular and thick septae
- Wilms’ tumors are believe to form malignant end of spectrum with cystic nephroma being benign and CPDN in between
Treatment
Complications
- Cyst herniation into the renal pelvis most frequent complication
Prognosis


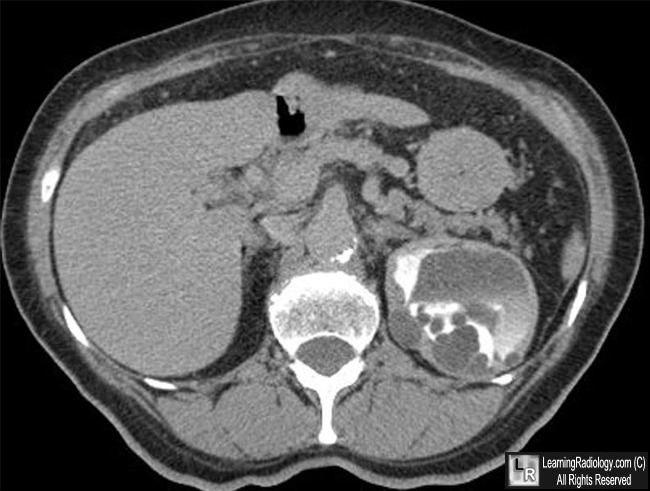
Cystic Nephroma. Two top images are coronal reconstructions from a contrast-enhanced CT urogram demonstrating a cystic mass in the upper pole (white arrows) of the left kidney that is septated and displacing the normal collecting system. The normal lower pole is shown by the red arrow. The axial CT image on the bottom shows the same lesion (white arrow) and the compressed collecting system (blue arrow)
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
\
eMedicine Multilocular Cystic Nephroma Lederman, H and Hurh, P.
|
|
|

{kind=link}
{kind=link}