|
|
Primary Sclerosing Cholangitis
PSC
General Considerations
- Inflammation, destruction and fibrosis of intrahepatic and extrahepatic bile ducts
- Unknown etiology but thought to be auto-immune
- A major cause of liver transplants in United States
- Majority occur in association with inflammatory bowel disease (IBD)
- Most often ulcerative colitis (UC)
- 5% of all patients with UC have PSC
- 75% of all patients with PSC will have UC
- Most often between 30-60 years of age with a mean of 40
Clinical Findings
- Asymptomatic; onset of symptoms is insidious
- Diarrhea
- Fever, chills
- Jaundice
- Pruritus
- Elevated serum alkaline phosphatase, aspartate aminotransferase and ascorbate levels
Imaging Findings
- ERCP considered study of choice but magnetic resonance cholangiopancreatography (MRCP) is less invasive and approaches accuracy of ERCP
- Early changes may include ulceration of the common bile duct
- Irregular narrowing with saccular dilatation proximal to strictured ducts leads to beaded (beads-on-a-string) appearance of ducts
- Usually involves intra- and extrahepatic ducts simultaneously
- MRCP findings
- High T2 in wedge-shaped areas with dilatation of ducts
- US may show thickening of gallbladder wall, thickening and dilatation of the bile ducts
Differential Diagnosis
- Secondary causes of cholangitis which can mimic PSC
Treatment
- Endoscopic dilatation of some strictures has been tried
- Definitive treatment is liver transplantation
Complications
- Cirrhosis
- Portal hypertension
- Liver failure (as long as 10-15 years after diagnosis)
- Cholangiocarcinoma
Prognosis


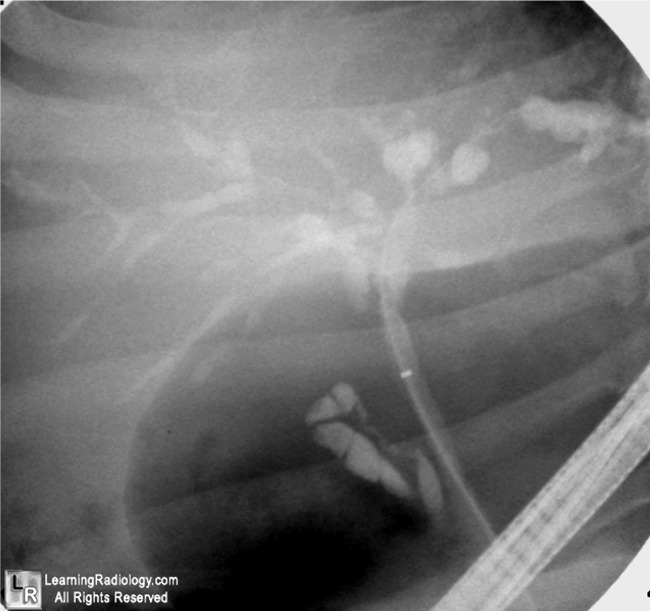
Primary Sclerosing Cholangitis. Images from Endoscopic Retrograde Cholangiopancreatography (ERCP) show alternating areas of stricture (black arrows) and dilated segments of the intrahepatic ducts (white arrows) characteristic of the "beaded" appearance seen with primary sclerosing cholangitis.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here and here
MedScape Primary Sclerosing Cholangitis -- Approach to Diagnosis Steele, I; Levy, C; Lindor, K
|
|
|

{kind=link}
{kind=link}