|
|
Epiploic Appendagitis
Appendicitis Epiploica
General Considerations
- Uncommon cause of acute abdominal pain
- Occurs most often in men in 4th and 5th decade
- Inflammation of epiploic appendages (appendices)
- Peritoneal outpouchings originating from serosal surface of colon
- Contain blood vessels and fat
- Diagnosis requires cross-sectional imaging
- Inflammation may be caused by venous occlusion
- “Secondary” epiploic appendagitis is caused by inflammation of an adjacent structure
Clinical Findings
- Findings resemble acute diverticulitis or appendicitis
- Usually left lower quadrant abdominal pain
- Fever is usually absent or mild
- White cell count is usually normal
- Vigorous exercise and obesity have been postulated as facilitating torsion of the appendage
Imaging Findings
- 1.5-3.5 cm fat density lesion with surrounding inflammatory changes
- Usually abuts anterior wall of sigmoid colon
- Central, high density focus within fat (54%)
- Probably thrombosed blood vessel
- Colon wall thickening is unusual
- Changes resolve within 6 months
- Occasionally, fat necrosis may lead to calcification of the appendage
- On US
- Echogenic ovoid mass at point of tenderness
- Hypoechoic ring (swelling of serosa)
Differential Diagnosis
- Mesenteric panniculitis

- Diverticulitis
- Trauma
- Neoplasm, e.g. liposarcoma
- Omental infarction
- Typically located in the right lower quadrant
- Between anterior abdominal wall and ascending or transverse colon
Treatment
- Conservative treatment with pain medication
- Symptoms subside within a week and CT scan returns to normal by 6 months
- Non-surgical
Complications
- Rarely, adhesions, obstruction, peritonitis, abscess formation
Prognosis
- Self-limited disease should result in complete resolution


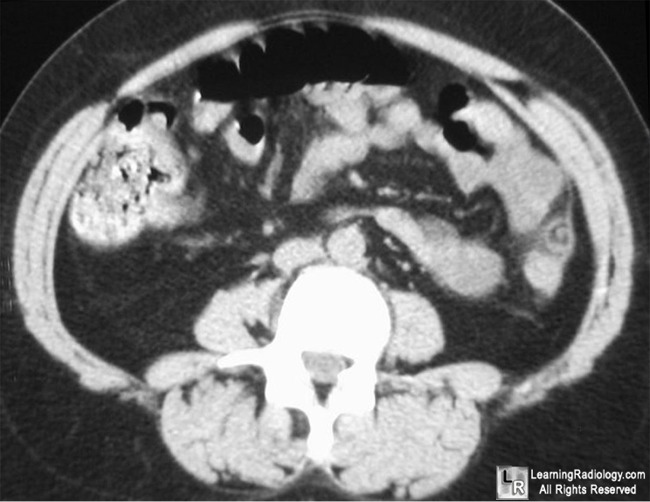
Epiploic Appendagitis. Two axial CT scans of the lower abdomen show the classical findings of an oval, fat-containing mass abutting the sigmoid colon (red arrow) with surrounding inflammatory stranding of the fate (red circle). There is a characteristic dense focus within the fatty density which may represent a thrombosed vessel or hemorrhage.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here and here
Singh, A; Gervais, D, Hahn, P, Rhea, J and Mueller, P. CT Appearance of Acute Appendagitis AJR 2004;183:1303–1307
Singh, A; Gervais, D, Hahn, P, Sagar, P, Mueller, P and Novelline, R. Acute Epiploic Appendagitis and Its Mimics RadioGraphics 2005;25:1521-1534
|
|
|

{kind=link}
{kind=link}