|
|
Dislocation of the Knee
General Considerations
- Uncommon dislocation
- Most are either anterior or posterior
- Using the position of the tibia as the reference
- Anterior dislocations (most frequent)
- Hyperextension
- Posterior dislocations (second most frequent)
- Force to anterior tibia with knee flexed as in MVC or falls
- Medial, lateral or rotational
- Valgus, varus or rotational forces
- As many as 50% of knee dislocations spontaneously self-reduce
- Can lead to underestimation of damage
- Most believe that dislocation requires injury to both anterior and posterior cruciate ligaments and either of the collateral ligaments
Clinical Findings
- Gross deformity
- Swelling
- Intense pain
Imaging Findings
- Conventional radiography is the study of choice
- MRI will demonstrate ligamentous injuries
- Fractures of tibial plateau are relatively common
- Also proximal fibula and tibial spines
Treatment
- Immediate closed reduction after full evaluation for associated injuries
- Surgical repair of ligamentous injuries is usually carried out several weeks after injury
Complications
- Co-existent vascular injuries
- Loss of limb
- Compound fractures are common (30%)
- Peroneal nerve injury
- Ligamentous injury
- Deep vein thrombosis
- Compartment syndrome
Prognosis
- High velocity injuries result in more damage and have a worse prognosis than low velocity injuries
- Most will regain full use of a stable knee


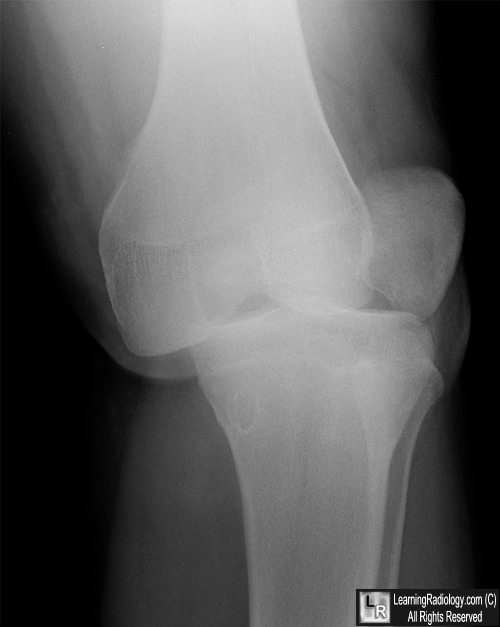
Posterior and Lateral Dislocation of Knee. The tibia is displaced laterally and posteriorly relative to the femur (red arrow). The patella is displaced laterally (black and white arrows) and comes to lie over the lateral femoral condyle. Some degree of rotational force is usually required to produce this type of injury.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here and here
Knee Dislocations eMedicine Green, J; Shahrdar, C; Owens, B
A Review of Knee Dislocations. Henrichs, A. Journal of Athletic Training 2004;39(4):365–369
|
|
|

{kind=link}
{kind=link}